También podría gustarte
- Hemodynamic Management Pocket Card PDFDocumento8 páginasHemodynamic Management Pocket Card PDFjenn1722Aún no hay calificaciones
- Common Cardiac MedicationsDocumento1 páginaCommon Cardiac MedicationsPaige HardekopfAún no hay calificaciones
- Bpacnz Antibiotics GuideDocumento40 páginasBpacnz Antibiotics GuideBulborea MihaelaAún no hay calificaciones
- CCRN Synergy and Exam StartegiesDocumento12 páginasCCRN Synergy and Exam StartegiesMarcus, RN100% (2)
- Critical Care Intravenous DrugsDocumento1 páginaCritical Care Intravenous DrugsMarynel Dixie Izon Brao89% (9)
- DRUG TITRATION GUIDEDocumento2 páginasDRUG TITRATION GUIDEEgi Munandar100% (1)
- Vasopressors and InotropesDocumento4 páginasVasopressors and InotropesSdAún no hay calificaciones
- Primary Care of Musculoskeletal Problems in The Outpatient SettingDocumento350 páginasPrimary Care of Musculoskeletal Problems in The Outpatient SettingMauriceGatto100% (1)
- CCRN-PCCN Review GastrointestinalDocumento23 páginasCCRN-PCCN Review GastrointestinalGiovanni MictilAún no hay calificaciones
- Ninja - Anti-HTN PDFDocumento6 páginasNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- DripsDocumento52 páginasDripsjanoloAún no hay calificaciones
- The Crash CartDocumento39 páginasThe Crash Cartpramod kumawat100% (1)
- ACLS Study Guide NewDocumento35 páginasACLS Study Guide NewNIRANJANA SHALINIAún no hay calificaciones
- Dimensional Analysis For Nursing StudentsDe EverandDimensional Analysis For Nursing StudentsAún no hay calificaciones
- ICU Guideline: Temporary Cardiac PacingDocumento8 páginasICU Guideline: Temporary Cardiac PacingistiAún no hay calificaciones
- Common ICU DripsDocumento1 páginaCommon ICU DripsSunshine Willis100% (2)
- Critical Care Guide covering Cardiac, Pulmonary, Infectious, Toxicology and Neurologic topicsDocumento150 páginasCritical Care Guide covering Cardiac, Pulmonary, Infectious, Toxicology and Neurologic topicsSylvia Gonzalez100% (2)
- ECG Master Class-2Documento138 páginasECG Master Class-2Shohag ID Center100% (1)
- Electrolyte CompleteDocumento6 páginasElectrolyte CompleteTofan Ana100% (2)
- Critical Care Note PDFDocumento10 páginasCritical Care Note PDFlml100% (1)
- Common Cardiac Drugs for Angina and StentingDocumento13 páginasCommon Cardiac Drugs for Angina and StentingDonna Deala100% (2)
- Pain Pocket GuideDocumento2 páginasPain Pocket Guidebtalera100% (2)
- ICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHDocumento32 páginasICU Drips: Stephanie Sanderson, RN, MSN, CNS, CCNS, CCRN Medical Cardiac ICU-UNMHNicole Adkins100% (1)
- DrugDocumento3 páginasDrugkhangsiean89100% (1)
- Icu NotesDocumento47 páginasIcu NotesChryst Louise SaavedraAún no hay calificaciones
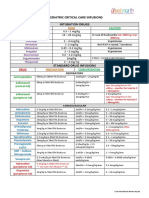
- Paediatric Critical Care Infusions Intubation DrugsDocumento2 páginasPaediatric Critical Care Infusions Intubation DrugsА. Сосорбарам100% (1)
- Dysrhythmia InterpretationDocumento56 páginasDysrhythmia InterpretationgerajassoAún no hay calificaciones
- ACLS Simulation ScenariosDocumento14 páginasACLS Simulation ScenariosVanessa HermioneAún no hay calificaciones
- Drug Card Emergency DepartmentDocumento2 páginasDrug Card Emergency Departmentdrmohdtanveer100% (3)
- Critical Care Calculations Study GuideDocumento6 páginasCritical Care Calculations Study GuideAja Blue100% (2)
- Adult Critical Care IV Medication Infusion SheetDocumento2 páginasAdult Critical Care IV Medication Infusion SheetPonchoi PintacasiAún no hay calificaciones
- ACLS Drugs&Drips Final PDFDocumento6 páginasACLS Drugs&Drips Final PDFmesrianti_rubenAún no hay calificaciones
- Cardiology Step 2 CK NotesDocumento5 páginasCardiology Step 2 CK NotesVidur S SinghAún no hay calificaciones
- ACLS PharmacologyDocumento5 páginasACLS PharmacologyKuruva MallikarjunaAún no hay calificaciones
- CNEA - CCRN Review - Behavioral-PsychosocialDocumento12 páginasCNEA - CCRN Review - Behavioral-PsychosocialalexAún no hay calificaciones
- Emergency Medical Procedures GuideDocumento57 páginasEmergency Medical Procedures GuideDuane Liloc100% (1)
- Drug Doses12Documento45 páginasDrug Doses12Asghar Shah100% (1)
- Medicine Haematology and DISEASESDocumento9 páginasMedicine Haematology and DISEASESrnvisAún no hay calificaciones
- Legal Medicine ReviewerDocumento47 páginasLegal Medicine ReviewerJoms KilgannonAún no hay calificaciones
- Drug Name Onset Concentration Dosing Instructions Drug Class How To TitrateDocumento1 páginaDrug Name Onset Concentration Dosing Instructions Drug Class How To Titrateje hanAún no hay calificaciones
- Emergency DrugsDocumento24 páginasEmergency Drugsourladymediatrixhospital hemodialysisunitAún no hay calificaciones
- ACLS Algorithms SlideDocumento26 páginasACLS Algorithms SlidehrsoAún no hay calificaciones
- ACLS Drugs: Primary Medications Used in Cardiac Arrest AlgorithmsDocumento10 páginasACLS Drugs: Primary Medications Used in Cardiac Arrest AlgorithmsChintami Octavia100% (1)
- Surgical Adult Critical Care Ref SheetDocumento3 páginasSurgical Adult Critical Care Ref Sheetsgod34100% (1)
- Ischemic Heart Disease: Definition, Pathophysiology, and EffectsDocumento10 páginasIschemic Heart Disease: Definition, Pathophysiology, and Effectsborn_321118403100% (1)
- Medications To KnowDocumento4 páginasMedications To KnowdtburrupAún no hay calificaciones
- FNP Resume Jenna Gibson 2022Documento2 páginasFNP Resume Jenna Gibson 2022api-619271904Aún no hay calificaciones
- Cardiac MedicationsDocumento8 páginasCardiac Medicationsangeline totaram100% (2)
- 209 Pope, B. CCRN-PCCN-CMC Review Cardiac Part 1Documento14 páginas209 Pope, B. CCRN-PCCN-CMC Review Cardiac Part 1peanant100% (1)
- Resuscitation MedicationDocumento1 páginaResuscitation MedicationDen SinyoAún no hay calificaciones
- Body Parts of A Frog and It's FunctionsDocumento3 páginasBody Parts of A Frog and It's FunctionsMichael ChuaAún no hay calificaciones
- EDAIC Part 2 Exams 2015, 2014, 2013Documento13 páginasEDAIC Part 2 Exams 2015, 2014, 2013dsdhaka50% (2)
- ACLS Official GuideDocumento11 páginasACLS Official GuideICU RSPGAún no hay calificaciones
- The Drug Doses in The Following Pages Are ReproducDocumento168 páginasThe Drug Doses in The Following Pages Are ReproducAsghar ShahAún no hay calificaciones
- ACAQ Crit Care Nursing CurriculumDocumento91 páginasACAQ Crit Care Nursing CurriculumAnne Julia Agustin100% (1)
- Cardiovascular SYSTEM - Heart Dysrythmia IllustrationsDocumento3 páginasCardiovascular SYSTEM - Heart Dysrythmia IllustrationsKim GonzalesAún no hay calificaciones
- Critical Care Drugs OverviewDocumento23 páginasCritical Care Drugs OverviewAsri Ernadi100% (1)
- Hemodynamics For The Bedside Nurse 1CEUDocumento7 páginasHemodynamics For The Bedside Nurse 1CEURN333100% (1)
- Critical CareDocumento40 páginasCritical Carenkuligowski100% (6)
- Farmakologi ICUDocumento54 páginasFarmakologi ICULin Phoponk100% (2)
- Sydenham's ChoreaDocumento17 páginasSydenham's ChoreaEmily EresumaAún no hay calificaciones
- FISA Club Training ProgrammeDocumento40 páginasFISA Club Training Programmemendes67Aún no hay calificaciones
- Bruce and Naughton ProtocolDocumento13 páginasBruce and Naughton ProtocolDheeraj RaiAún no hay calificaciones
- Pcap D, CHF 2 CHDDocumento78 páginasPcap D, CHF 2 CHDtrew_wertAún no hay calificaciones
- Cambridge O Level: BIOLOGY 5090/01Documento16 páginasCambridge O Level: BIOLOGY 5090/01Syed Ashar100% (1)
- CHD Managemen Withot Surgery Cansy JHC (Prof. Mul) PDFDocumento39 páginasCHD Managemen Withot Surgery Cansy JHC (Prof. Mul) PDFFery NurjayantoAún no hay calificaciones
- Question BankDocumento6 páginasQuestion Bankkoang lual gachAún no hay calificaciones
- Howtotreatrightheart Failure - Tipsforclinicians IneverydaypracticeDocumento11 páginasHowtotreatrightheart Failure - Tipsforclinicians IneverydaypracticesaqqarazoserAún no hay calificaciones
- Exercise For FitnessDocumento18 páginasExercise For FitnessJM Buhisan Acaso100% (1)
- Cat Dissection ProjectDocumento12 páginasCat Dissection Projectapi-309363754Aún no hay calificaciones
- Anaphy SGD HeartDocumento1 páginaAnaphy SGD HeartbrylleAún no hay calificaciones
- High Risk Consent For PCIDocumento1 páginaHigh Risk Consent For PCISree Sowjanya PatibandlaAún no hay calificaciones
- Growth Adaptations, Cell Death, and Hemostatic DisordersDocumento19 páginasGrowth Adaptations, Cell Death, and Hemostatic DisordersJustine Val RevalidaAún no hay calificaciones
- CVS ExaminationDocumento4 páginasCVS ExaminationGuruprasanth PazhamalaiAún no hay calificaciones
- 2020 Canadian Cardiovascular SocietyCanadian Heart Rhythm Society Position Statement On The Management of Ventricular Tachycardia and Fibrillation in Patients With Structural Heart Disease PDFDocumento15 páginas2020 Canadian Cardiovascular SocietyCanadian Heart Rhythm Society Position Statement On The Management of Ventricular Tachycardia and Fibrillation in Patients With Structural Heart Disease PDFDiego MerchánAún no hay calificaciones
- Aerobic Lab ReportDocumento16 páginasAerobic Lab Reportapi-502029423Aún no hay calificaciones
- Mitral Annular Disjunction: A Systematic Review of The LiteratureDocumento10 páginasMitral Annular Disjunction: A Systematic Review of The LiteratureAlznoskillAún no hay calificaciones
- Transport SystemDocumento22 páginasTransport Systemredditor1276Aún no hay calificaciones
- Krok 2- 2013מסומן (General Medicine)Documento26 páginasKrok 2- 2013מסומן (General Medicine)Nicole VinnikAún no hay calificaciones
- PHARMAfdDocumento7 páginasPHARMAfdJobelle AcenaAún no hay calificaciones
- Nejmra 2000348Documento16 páginasNejmra 2000348Mathew McCarthyAún no hay calificaciones
- ANATOM 128 Brochure-ReDocumento8 páginasANATOM 128 Brochure-ReAli MirzaAún no hay calificaciones
- Dysrhythmia TestsDocumento3 páginasDysrhythmia TestsKimberly WhitesideAún no hay calificaciones
- 48 Hour ChickDocumento13 páginas48 Hour ChickJowi SalAún no hay calificaciones