También podría gustarte
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2102)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Questions Related To CodesDocumento10 páginasQuestions Related To CodesMayur Mandrekar100% (1)
- New Age GeneratorDocumento26 páginasNew Age GeneratorDaud Ahmed Fihawango100% (1)
- LEEDDocumento161 páginasLEEDjeruelAún no hay calificaciones
- ITCC in Riyadh Residential Complex J10-13300 16715-1 Voice & Data Communication CablingDocumento16 páginasITCC in Riyadh Residential Complex J10-13300 16715-1 Voice & Data Communication CablinguddinnadeemAún no hay calificaciones
- Peter H. Rossi - Mark W. Lipsey - Howard E. Freeman - Evaluation - A Systematic ApproachDocumento417 páginasPeter H. Rossi - Mark W. Lipsey - Howard E. Freeman - Evaluation - A Systematic ApproachHector Urzua50% (2)
- Kim Lighting Landscape Lighting Catalog 1988Documento28 páginasKim Lighting Landscape Lighting Catalog 1988Alan MastersAún no hay calificaciones
- LeasingDocumento18 páginasLeasingsunithakravi0% (1)
- CFM56 3Documento148 páginasCFM56 3manmohan100% (1)
- 16 Times When History Turned Hilarious, #5 Is So Funny: 1. On The High! Hangover On Mind!Documento9 páginas16 Times When History Turned Hilarious, #5 Is So Funny: 1. On The High! Hangover On Mind!nahoAún no hay calificaciones
- m2l10 Lesson 10 The Force Method of Analysis: TrussesDocumento17 páginasm2l10 Lesson 10 The Force Method of Analysis: TrussesVitor ValeAún no hay calificaciones
- LM 004 Chp04.qxd PDFDocumento14 páginasLM 004 Chp04.qxd PDFnahoAún no hay calificaciones
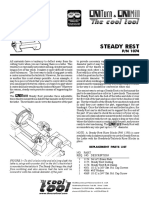
- Steady Rest: P/N 1074 P/N 1074 P/N 1074 P/N 1074 P/N 1074Documento1 páginaSteady Rest: P/N 1074 P/N 1074 P/N 1074 P/N 1074 P/N 1074nahoAún no hay calificaciones
- Topic6NestedForLoops 4up PDFDocumento6 páginasTopic6NestedForLoops 4up PDFBayu Agung Prakoso100% (1)
- 1032 L8Documento23 páginas1032 L8nahoAún no hay calificaciones
- 1032 L8Documento23 páginas1032 L8nahoAún no hay calificaciones
- Tended Range Sixteen Channel Supervised Stationary ReceiverDocumento2 páginasTended Range Sixteen Channel Supervised Stationary ReceiverAimee chaconAún no hay calificaciones
- Silicon Epitaxial Planar Transistor 2SA1179: Galaxy ElectricalDocumento5 páginasSilicon Epitaxial Planar Transistor 2SA1179: Galaxy ElectricalsacralAún no hay calificaciones
- Dr. Shekhar Challa Joins Bioscience Americas Board of AdvisorsDocumento2 páginasDr. Shekhar Challa Joins Bioscience Americas Board of AdvisorsPR.comAún no hay calificaciones
- DR - Vyshnavi Ts ResumeDocumento2 páginasDR - Vyshnavi Ts ResumeSuraj SingriAún no hay calificaciones
- English The RainDocumento2 páginasEnglish The RainsmitaAún no hay calificaciones
- Daftar Pustaka ProposalDocumento4 páginasDaftar Pustaka ProposalraniAún no hay calificaciones
- Kf22Qt Sec4 FRDDocumento21 páginasKf22Qt Sec4 FRDMauro PerezAún no hay calificaciones
- O/W: Mayne To Reward The Willing: Mayne Pharma Group (MYX)Documento8 páginasO/W: Mayne To Reward The Willing: Mayne Pharma Group (MYX)Muhammad ImranAún no hay calificaciones
- Imteyaz ResumeDocumento2 páginasImteyaz ResumeImteyaz AhmadAún no hay calificaciones
- Passive In-Line Chlorination For Drinking Water DiDocumento18 páginasPassive In-Line Chlorination For Drinking Water DitefovAún no hay calificaciones
- Report On Laxmi Niwas PalaceDocumento72 páginasReport On Laxmi Niwas PalaceRenu MahayachAún no hay calificaciones
- Hindustan Coca-Cola Beverages PVT LTD B-91 Mayapuri Industrial Area Phase-I New DelhiDocumento2 páginasHindustan Coca-Cola Beverages PVT LTD B-91 Mayapuri Industrial Area Phase-I New DelhiUtkarsh KadamAún no hay calificaciones
- Soc5352 1331Documento4 páginasSoc5352 1331ChinAún no hay calificaciones
- Leon County Sheriff'S Office Daily Booking Report 18-Oct-2020 Page 1 of 3Documento3 páginasLeon County Sheriff'S Office Daily Booking Report 18-Oct-2020 Page 1 of 3WCTV Digital TeamAún no hay calificaciones
- Components of FitnessDocumento3 páginasComponents of Fitnessapi-3830277100% (1)
- Effect of Educational Environment On Personality and Adjustment of Female Students Studying in Colleges of UttarakhandDocumento5 páginasEffect of Educational Environment On Personality and Adjustment of Female Students Studying in Colleges of UttarakhandESSENCE - International Journal for Environmental Rehabilitation and ConservaionAún no hay calificaciones
- Mouse HardyweinbergDocumento5 páginasMouse Hardyweinbergapi-477617112Aún no hay calificaciones
- Synergic Antiobesity Effects of Bitter Melon Water Extract and Platycodin-D in Genetically Obese MiceDocumento9 páginasSynergic Antiobesity Effects of Bitter Melon Water Extract and Platycodin-D in Genetically Obese Micegege wpAún no hay calificaciones
- Denon DHT-T100 Ver 3 PDFDocumento34 páginasDenon DHT-T100 Ver 3 PDFboroda241083% (6)
- Important Topics RTCDocumento18 páginasImportant Topics RTCjoydeep12Aún no hay calificaciones
- SECTION 02892 Traffic Signals Rev 0Documento65 páginasSECTION 02892 Traffic Signals Rev 0Abdul HannanAún no hay calificaciones
- SWT Nedelka Cartagena enDocumento2 páginasSWT Nedelka Cartagena enChristian Lazo FerreyraAún no hay calificaciones