También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
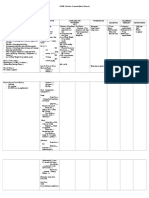
- Wound Assessment ChartDocumento2 páginasWound Assessment ChartAnonymous H3DpmCZX100% (6)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- An Extract From Meg Wolitzer's BelzharDocumento20 páginasAn Extract From Meg Wolitzer's BelzharSimonKidsUK0% (4)
- Proposal Kegiatan Daerah Binaan Imku: Presented byDocumento1 páginaProposal Kegiatan Daerah Binaan Imku: Presented byAditya IslamiAún no hay calificaciones
- DT - Focussed Assesment Sonography in TraumaDocumento19 páginasDT - Focussed Assesment Sonography in TraumaAditya IslamiAún no hay calificaciones
- POMR 2. Lung TumourDocumento3 páginasPOMR 2. Lung TumourAditya IslamiAún no hay calificaciones
- Urinary Tract Stones: Aditya Islami Kepaniteraan Klinik Ilmu Bedah Pembimbing: Dr. Rantapina Kurnia Sari, SP.BDocumento3 páginasUrinary Tract Stones: Aditya Islami Kepaniteraan Klinik Ilmu Bedah Pembimbing: Dr. Rantapina Kurnia Sari, SP.BAditya IslamiAún no hay calificaciones
- Complications of Total Knee Arthroplasty: Standardized List and Definitions of The Knee SocietyDocumento6 páginasComplications of Total Knee Arthroplasty: Standardized List and Definitions of The Knee SocietyotakmesumAún no hay calificaciones
- 2 NICU Nurse Resume TemplateDocumento1 página2 NICU Nurse Resume TemplateMohamed AbodaifAún no hay calificaciones
- 1971 WL 126685Documento142 páginas1971 WL 126685Thalia SandersAún no hay calificaciones
- DR Form BsuDocumento1 páginaDR Form BsumingcatAún no hay calificaciones
- Nursing Record and ReportsDocumento32 páginasNursing Record and ReportsOm VaishNav100% (1)
- Harrison Bill Reba 1981 Rhodesia PDFDocumento4 páginasHarrison Bill Reba 1981 Rhodesia PDFthe missions networkAún no hay calificaciones
- Ra 9288Documento8 páginasRa 9288UlaysaAún no hay calificaciones
- Daniel Ward Application Portland Police Brutality Community Liaison ApplicationDocumento15 páginasDaniel Ward Application Portland Police Brutality Community Liaison Applicationmary engAún no hay calificaciones
- Role Play Ambulation: Group 4Documento5 páginasRole Play Ambulation: Group 4diana ratriAún no hay calificaciones
- KONSELING DOSEN Beginning A RelationshipDocumento30 páginasKONSELING DOSEN Beginning A RelationshipfaiqAún no hay calificaciones
- SwotDocumento3 páginasSwotKimberley Anne SantosAún no hay calificaciones
- TPH Quality Assurance PolicyDocumento8 páginasTPH Quality Assurance PolicyAl Sah HimAún no hay calificaciones
- Tcharestresumefinal 1009Documento2 páginasTcharestresumefinal 1009tcharestAún no hay calificaciones
- CGHS HospitalsDocumento9 páginasCGHS Hospitalsgarg_mahak3199Aún no hay calificaciones
- Ueropass CV Format.Documento4 páginasUeropass CV Format.kennagy2000Aún no hay calificaciones
- Reported SpeechDocumento3 páginasReported SpeechReka KutasiAún no hay calificaciones
- ADM. Case No. 7897Documento6 páginasADM. Case No. 7897Judge Florentino FloroAún no hay calificaciones
- 50 Item Psychiatric Nursing Exam IDocumento11 páginas50 Item Psychiatric Nursing Exam Iɹǝʍdןnos98% (40)
- Hob BitDocumento2 páginasHob BitShebl RamadanAún no hay calificaciones
- CRICO/RMF's Breast Care Management Algorithm Back To TopDocumento2 páginasCRICO/RMF's Breast Care Management Algorithm Back To Topsavvy_as_98Aún no hay calificaciones
- Jewish Standard, September 28, 2018Documento92 páginasJewish Standard, September 28, 2018New Jersey Jewish StandardAún no hay calificaciones
- Assignment!: Complete The SentencesDocumento3 páginasAssignment!: Complete The SentencesFiska Maida100% (1)
- Marissa Hamby Resume Final DraftDocumento2 páginasMarissa Hamby Resume Final Draftapi-353698203Aún no hay calificaciones
- Institute of Research and Burn Hospital in BahawalpurDocumento10 páginasInstitute of Research and Burn Hospital in BahawalpurHamid RehmanAún no hay calificaciones
- The Role of Community Mental Health Teams in Delivering Community Mental Health Services Guidance PDFDocumento23 páginasThe Role of Community Mental Health Teams in Delivering Community Mental Health Services Guidance PDFEno RLAún no hay calificaciones
- Hospital ProfileDocumento3 páginasHospital ProfilePrakruti Care Hospital & IccuAún no hay calificaciones
- The Exercise On The Simple Present TenseDocumento3 páginasThe Exercise On The Simple Present TensecintyaAún no hay calificaciones
- The Miracle Man Chapters 1 22Documento37 páginasThe Miracle Man Chapters 1 22Utkarsha KesarkarAún no hay calificaciones