También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Undergraduate Medicine Study Notes PDFDocumento764 páginasUndergraduate Medicine Study Notes PDFSHAKEEL1991Aún no hay calificaciones
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Public Access - The GauntletDocumento1 páginaPublic Access - The GauntletTesting0% (2)
- Mark Magazine#65Documento196 páginasMark Magazine#65AndrewKanischevAún no hay calificaciones
- A - PAGE 1 - MergedDocumento73 páginasA - PAGE 1 - MergedGenalyn DomantayAún no hay calificaciones
- Test - 4 Intensive Therapy of Somatic Complicaton. Cardio Pulmonary Resuscitation (CPR)Documento6 páginasTest - 4 Intensive Therapy of Somatic Complicaton. Cardio Pulmonary Resuscitation (CPR)Isak ShatikaAún no hay calificaciones
- Test - 13 Odontogenic Osteomyelitis of The Jaws, Furuncles, Carbuncles, ErysipelasDocumento5 páginasTest - 13 Odontogenic Osteomyelitis of The Jaws, Furuncles, Carbuncles, ErysipelasIsak ShatikaAún no hay calificaciones
- Test - 20 Dental ImplantsDocumento5 páginasTest - 20 Dental ImplantsIsak ShatikaAún no hay calificaciones
- CV Example - 2019 Issak1Documento3 páginasCV Example - 2019 Issak1Isak ShatikaAún no hay calificaciones
- Test - 14 Diseases of The TMJ PDFDocumento4 páginasTest - 14 Diseases of The TMJ PDFIsak ShatikaAún no hay calificaciones
- Test - 18 Specific Diseases - Actinomycosis, TB, Syphilis, HIVDocumento4 páginasTest - 18 Specific Diseases - Actinomycosis, TB, Syphilis, HIVIsak ShatikaAún no hay calificaciones
- Test - 12 Odontogenic Maxillary SinusitisDocumento5 páginasTest - 12 Odontogenic Maxillary SinusitisIsak ShatikaAún no hay calificaciones
- Test - 9 Chronic PeriodontitisDocumento5 páginasTest - 9 Chronic PeriodontitisIsak ShatikaAún no hay calificaciones
- Test - 8 Retension, Dystopia, PericoronitisDocumento5 páginasTest - 8 Retension, Dystopia, PericoronitisIsak ShatikaAún no hay calificaciones
- Test - 6 Methods of Extractions (Tooth Removal)Documento4 páginasTest - 6 Methods of Extractions (Tooth Removal)Isak ShatikaAún no hay calificaciones
- Schedule Classes 4th Years Ist SemesterDocumento1 páginaSchedule Classes 4th Years Ist SemesterIsak ShatikaAún no hay calificaciones
- Salmon Ellos IsDocumento5 páginasSalmon Ellos IsIsak ShatikaAún no hay calificaciones
- Schedule Classes 5th Years 1st SemesterDocumento1 páginaSchedule Classes 5th Years 1st SemesterIsak ShatikaAún no hay calificaciones
- TularemiaDocumento5 páginasTularemiaIsak ShatikaAún no hay calificaciones
- Viral Hepatitis (Part II)Documento10 páginasViral Hepatitis (Part II)Isak ShatikaAún no hay calificaciones
- Test - 10 Root (Radicular) CystsDocumento5 páginasTest - 10 Root (Radicular) CystsIsak ShatikaAún no hay calificaciones
- Lecture: Erysipelas: Basic Clinical PrinciplesDocumento15 páginasLecture: Erysipelas: Basic Clinical PrinciplesIsak ShatikaAún no hay calificaciones
- Short Table of Infectious DiseasesDocumento9 páginasShort Table of Infectious DiseasesIsak ShatikaAún no hay calificaciones
- Food Poisoning: Major Infectious Causes of Acute DiarrheaDocumento7 páginasFood Poisoning: Major Infectious Causes of Acute DiarrheaIsak ShatikaAún no hay calificaciones
- Cases InfectiousDocumento20 páginasCases InfectiousIsak ShatikaAún no hay calificaciones
- Yersiniosis: Yersinia Pathogenic Kinds and VariantsDocumento7 páginasYersiniosis: Yersinia Pathogenic Kinds and VariantsIsak ShatikaAún no hay calificaciones
- Chapter 3. Clinical Forms of Tuberculosis: Tuberculosis Course For English-Speaking StudentsDocumento20 páginasChapter 3. Clinical Forms of Tuberculosis: Tuberculosis Course For English-Speaking StudentsIsak ShatikaAún no hay calificaciones
- Cases InfectiousDocumento20 páginasCases InfectiousIsak ShatikaAún no hay calificaciones
- 00 0 Etio All 2014 - 1 PDFDocumento88 páginas00 0 Etio All 2014 - 1 PDFIsak ShatikaAún no hay calificaciones
- Chapter 3. Clinical Forms of Tuberculosis 3.1. Tubercular IntoxicationDocumento14 páginasChapter 3. Clinical Forms of Tuberculosis 3.1. Tubercular IntoxicationIsak ShatikaAún no hay calificaciones
- Juvenile Rheumatoid ArthritisDocumento10 páginasJuvenile Rheumatoid ArthritisIsak ShatikaAún no hay calificaciones
- 2.5. The Identification Of Мвт Drug Resistance: Tuberculosis Course for English-speaking studentsDocumento9 páginas2.5. The Identification Of Мвт Drug Resistance: Tuberculosis Course for English-speaking studentsIsak ShatikaAún no hay calificaciones
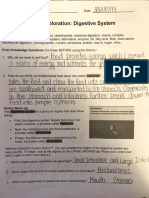
- Student Exploration: Digestive System: Food Inio Simple Nutrien/oDocumento9 páginasStudent Exploration: Digestive System: Food Inio Simple Nutrien/oAshantiAún no hay calificaciones
- Geometry and IntuitionDocumento9 páginasGeometry and IntuitionHollyAún no hay calificaciones
- Project Manager PMP PMO in Houston TX Resume Nicolaas JanssenDocumento4 páginasProject Manager PMP PMO in Houston TX Resume Nicolaas JanssenNicolaasJanssenAún no hay calificaciones
- Historical Exchange Rates - OANDA AUD-MYRDocumento1 páginaHistorical Exchange Rates - OANDA AUD-MYRML MLAún no hay calificaciones
- Bajaj CNSDocumento3 páginasBajaj CNSAbhijit PaikarayAún no hay calificaciones
- Suspend and Resume Calls: Exit PlugDocumento4 páginasSuspend and Resume Calls: Exit PlugrajuAún no hay calificaciones
- Bushcraft Knife AnatomyDocumento2 páginasBushcraft Knife AnatomyCristian BotozisAún no hay calificaciones
- Financial Accounting 1: Chapter 5 Cash and Short Term InvestmentDocumento31 páginasFinancial Accounting 1: Chapter 5 Cash and Short Term InvestmentCabdiraxmaan GeeldoonAún no hay calificaciones
- ICD10WHO2007 TnI4Documento1656 páginasICD10WHO2007 TnI4Kanok SongprapaiAún no hay calificaciones
- Principles of Business Grade 10 June 2021 Time: 1 1/2 Hrs. Paper 2 Answer ONLY 1 Question in Section I. Section IDocumento3 páginasPrinciples of Business Grade 10 June 2021 Time: 1 1/2 Hrs. Paper 2 Answer ONLY 1 Question in Section I. Section Iapi-556426590Aún no hay calificaciones
- Q4 Music 6 Module 2Documento15 páginasQ4 Music 6 Module 2Dan Paolo AlbintoAún no hay calificaciones
- Product Specifications Product Specifications: LLPX411F LLPX411F - 00 - V1 V1Documento4 páginasProduct Specifications Product Specifications: LLPX411F LLPX411F - 00 - V1 V1David MooneyAún no hay calificaciones
- Addition Color by Code: Yellow 1, 2, Blue 3, 4, Pink 5, 6 Peach 7, 8 Light Green 9, 10, Black 11Documento1 páginaAddition Color by Code: Yellow 1, 2, Blue 3, 4, Pink 5, 6 Peach 7, 8 Light Green 9, 10, Black 11Noor NadhirahAún no hay calificaciones
- Specialty Coffee Association of Indonesia Cupping Form (ARABICA)Documento1 páginaSpecialty Coffee Association of Indonesia Cupping Form (ARABICA)Saiffullah RaisAún no hay calificaciones
- Britannia Volume 12 Issue 1981 (Doi 10.2307/526240) Michael P. Speidel - Princeps As A Title For 'Ad Hoc' CommandersDocumento8 páginasBritannia Volume 12 Issue 1981 (Doi 10.2307/526240) Michael P. Speidel - Princeps As A Title For 'Ad Hoc' CommandersSteftyraAún no hay calificaciones
- BRAND AWARENESS Proposal DocumentDocumento11 páginasBRAND AWARENESS Proposal DocumentBuchi MadukaAún no hay calificaciones
- Contoh Assignment PDFDocumento18 páginasContoh Assignment PDFSiti Fatimah A Salam67% (3)
- Electric Vehicles PresentationDocumento10 páginasElectric Vehicles PresentationVIBHU CHANDRANSH BHANOT100% (1)
- LKG Math Question Paper: 1. Count and Write The Number in The BoxDocumento6 páginasLKG Math Question Paper: 1. Count and Write The Number in The BoxKunal Naidu60% (5)
- 200150, 200155 & 200157 Accelerometers: DescriptionDocumento16 páginas200150, 200155 & 200157 Accelerometers: DescriptionJOSE MARIA DANIEL CANALESAún no hay calificaciones
- Lesson: The Averys Have Been Living in New York Since The Late NinetiesDocumento1 páginaLesson: The Averys Have Been Living in New York Since The Late NinetiesLinea SKDAún no hay calificaciones
- List of Phrasal Verbs 1 ColumnDocumento12 páginasList of Phrasal Verbs 1 ColumnmoiibdAún no hay calificaciones
- Villamaria JR Vs CADocumento2 páginasVillamaria JR Vs CAClarissa SawaliAún no hay calificaciones
- 1 - Laminar and Turbulent Flow - MITWPU - HP - CDK PDFDocumento13 páginas1 - Laminar and Turbulent Flow - MITWPU - HP - CDK PDFAbhishek ChauhanAún no hay calificaciones
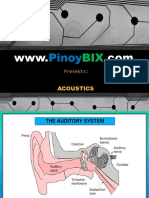
- AcousticsDocumento122 páginasAcousticsEclipse YuAún no hay calificaciones
- PH of Soils: Standard Test Method ForDocumento3 páginasPH of Soils: Standard Test Method ForYizel CastañedaAún no hay calificaciones
- Metalcor - 1.4507 - Alloy - F255 - Uranus 52N - S32520Documento1 páginaMetalcor - 1.4507 - Alloy - F255 - Uranus 52N - S32520NitinAún no hay calificaciones