También podría gustarte
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- Sample Opposition To Motion To Strike Portions of Complaint in United States District CourtDocumento2 páginasSample Opposition To Motion To Strike Portions of Complaint in United States District CourtStan Burman100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- SGBV SopDocumento72 páginasSGBV SopMigori ArtAún no hay calificaciones
- Disaster Recovery Plan STDocumento14 páginasDisaster Recovery Plan STMigori ArtAún no hay calificaciones
- Co Operative Bank Codes As of April 2014 PDFDocumento29 páginasCo Operative Bank Codes As of April 2014 PDFMigori Art0% (2)
- WHO Lab Quality Management SystemDocumento246 páginasWHO Lab Quality Management SystemMigori Art100% (1)
- 1934 PARIS AIRSHOW REPORT - Part1 PDFDocumento11 páginas1934 PARIS AIRSHOW REPORT - Part1 PDFstarsalingsoul8000Aún no hay calificaciones
- Quality Policy Manual V3 PDF 15 122011Documento82 páginasQuality Policy Manual V3 PDF 15 122011Migori Art100% (5)
- 450i User ManualDocumento54 páginas450i User ManualThượng Lê Văn0% (2)
- State Immunity Cases With Case DigestsDocumento37 páginasState Immunity Cases With Case DigestsStephanie Dawn Sibi Gok-ong100% (4)
- Advertisement KMTC 2019.2020. CleanedDocumento2 páginasAdvertisement KMTC 2019.2020. CleanedMigori ArtAún no hay calificaciones
- Aar Insurance New in Patient Preauthorization Form 2019Documento1 páginaAar Insurance New in Patient Preauthorization Form 2019Migori Art0% (2)
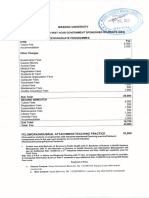
- Fees Structure For FreshersDocumento8 páginasFees Structure For FreshersMigori ArtAún no hay calificaciones
- Process MapDocumento1 páginaProcess MapMigori ArtAún no hay calificaciones
- PrEP - A Toolkit For Providers - InspectionCopy - March17Documento37 páginasPrEP - A Toolkit For Providers - InspectionCopy - March17Migori ArtAún no hay calificaciones
- Introduction & Epidemiology of TBDocumento45 páginasIntroduction & Epidemiology of TBMigori ArtAún no hay calificaciones
- Active Case FindingDocumento23 páginasActive Case FindingMigori ArtAún no hay calificaciones
- Fighting Pseudoscience Isn't Free: We Believe We Play An Important Role in Defending Truth and ObjectivityDocumento20 páginasFighting Pseudoscience Isn't Free: We Believe We Play An Important Role in Defending Truth and ObjectivityMigori ArtAún no hay calificaciones
- Lab Diagnosis of TBDocumento73 páginasLab Diagnosis of TBMigori ArtAún no hay calificaciones
- Kenya Natl Guidelines On MGMT of Sexual Violence 3rd Edition 2014Documento98 páginasKenya Natl Guidelines On MGMT of Sexual Violence 3rd Edition 2014Migori ArtAún no hay calificaciones
- Pep Protocol 2016Documento2 páginasPep Protocol 2016Migori ArtAún no hay calificaciones
- Accreditation Report.Documento1 páginaAccreditation Report.Migori ArtAún no hay calificaciones
- Guidelines For The Management of Drug Resistant Tuberculosis in Kenya (2010)Documento88 páginasGuidelines For The Management of Drug Resistant Tuberculosis in Kenya (2010)Migori ArtAún no hay calificaciones
- Counsellingthe Cancerpatient: Surgeon'Scounsel : George T. Pack, M.DDocumento5 páginasCounsellingthe Cancerpatient: Surgeon'Scounsel : George T. Pack, M.DMigori ArtAún no hay calificaciones
- Knbts-Blood Donation GuidelinesDocumento10 páginasKnbts-Blood Donation GuidelinesMigori ArtAún no hay calificaciones
- Genetically Modified Organis1Documento17 páginasGenetically Modified Organis1Migori ArtAún no hay calificaciones
- Kenya NationalPolicyoninjectionDocumento18 páginasKenya NationalPolicyoninjectionMigori ArtAún no hay calificaciones
- Ipc GuidelinesDocumento210 páginasIpc GuidelinesMigori ArtAún no hay calificaciones
- Specimen Referral Networks FinalDocumento132 páginasSpecimen Referral Networks FinalMigori ArtAún no hay calificaciones
- Adherence Counseling and Treatment Preparation SopDocumento47 páginasAdherence Counseling and Treatment Preparation SopMigori Art100% (1)
- Kenya Health Sector Referal StrategyDocumento64 páginasKenya Health Sector Referal StrategyMigori ArtAún no hay calificaciones
- CCC No: Ministry of Health Effective 01 October 2016 Viral Load Requisition FormDocumento1 páginaCCC No: Ministry of Health Effective 01 October 2016 Viral Load Requisition FormMigori ArtAún no hay calificaciones
- Kenya Health Policy 2014 2030Documento87 páginasKenya Health Policy 2014 2030Migori ArtAún no hay calificaciones
- Optimization of ART RegimenDocumento81 páginasOptimization of ART RegimenMigori Art100% (1)
- 1400 Service Manual2Documento40 páginas1400 Service Manual2Gabriel Catanescu100% (1)
- Ts Us Global Products Accesories Supplies New Docs Accessories Supplies Catalog916cma - PDFDocumento308 páginasTs Us Global Products Accesories Supplies New Docs Accessories Supplies Catalog916cma - PDFSRMPR CRMAún no hay calificaciones
- BluetoothDocumento28 páginasBluetoothMilind GoratelaAún no hay calificaciones
- Danby Dac5088m User ManualDocumento12 páginasDanby Dac5088m User ManualElla MariaAún no hay calificaciones
- Forecasting of Nonlinear Time Series Using Artificial Neural NetworkDocumento9 páginasForecasting of Nonlinear Time Series Using Artificial Neural NetworkranaAún no hay calificaciones
- Supergrowth PDFDocumento9 páginasSupergrowth PDFXavier Alexen AseronAún no hay calificaciones
- Doas - MotorcycleDocumento2 páginasDoas - MotorcycleNaojAún no hay calificaciones
- PeopleSoft Application Engine Program PDFDocumento17 páginasPeopleSoft Application Engine Program PDFSaurabh MehtaAún no hay calificaciones
- Rating SheetDocumento3 páginasRating SheetShirwin OliverioAún no hay calificaciones
- General Financial RulesDocumento9 páginasGeneral Financial RulesmskAún no hay calificaciones
- SM Land Vs BCDADocumento68 páginasSM Land Vs BCDAelobeniaAún no hay calificaciones
- 199437-Unit 4Documento36 páginas199437-Unit 4Yeswanth rajaAún no hay calificaciones
- Web Technology PDFDocumento3 páginasWeb Technology PDFRahul Sachdeva100% (1)
- Algorithmique Et Programmation en C: Cours Avec 200 Exercices CorrigésDocumento298 páginasAlgorithmique Et Programmation en C: Cours Avec 200 Exercices CorrigésSerges KeouAún no hay calificaciones
- Capital Expenditure DecisionDocumento10 páginasCapital Expenditure DecisionRakesh GuptaAún no hay calificaciones
- LMU-2100™ Gprs/Cdmahspa Series: Insurance Tracking Unit With Leading TechnologiesDocumento2 páginasLMU-2100™ Gprs/Cdmahspa Series: Insurance Tracking Unit With Leading TechnologiesRobert MateoAún no hay calificaciones
- ESG NotesDocumento16 páginasESG Notesdhairya.h22Aún no hay calificaciones
- ARUP Project UpdateDocumento5 páginasARUP Project UpdateMark Erwin SalduaAún no hay calificaciones
- Epidemiologi DialipidemiaDocumento5 páginasEpidemiologi DialipidemianurfitrizuhurhurAún no hay calificaciones
- Cryo EnginesDocumento6 páginasCryo EnginesgdoninaAún no hay calificaciones
- Working Capital ManagementDocumento39 páginasWorking Capital ManagementRebelliousRascalAún no hay calificaciones
- Aisladores 34.5 KV Marca Gamma PDFDocumento8 páginasAisladores 34.5 KV Marca Gamma PDFRicardo MotiñoAún no hay calificaciones
- Hager Pricelist May 2014Documento64 páginasHager Pricelist May 2014rajinipre-1Aún no hay calificaciones
- Ucm6510 Usermanual PDFDocumento393 páginasUcm6510 Usermanual PDFCristhian ArecoAún no hay calificaciones
- Shubham Tonk - ResumeDocumento2 páginasShubham Tonk - ResumerajivAún no hay calificaciones
- Specialty Arc Fusion Splicer: FSM-100 SeriesDocumento193 páginasSpecialty Arc Fusion Splicer: FSM-100 SeriesSFTB SoundsFromTheBirdsAún no hay calificaciones