También podría gustarte
- The Number of Variants in The Greek - New TestamentDocumento16 páginasThe Number of Variants in The Greek - New Testamenthudson1963100% (1)
- The Number of Variants in The Greek - New TestamentDocumento16 páginasThe Number of Variants in The Greek - New Testamenthudson1963100% (1)
- Explanatory Supplement Astronomical Almanac PDFDocumento394 páginasExplanatory Supplement Astronomical Almanac PDFsrks9999100% (4)
- Suetonius Vol 2 (Loeb)Documento571 páginasSuetonius Vol 2 (Loeb)Sarai Iehanne van BeeuwelanAún no hay calificaciones
- Guidelines For Interconfessional CooperationDocumento12 páginasGuidelines For Interconfessional Cooperationhudson1963Aún no hay calificaciones
- The Zoot Suit RiotDocumento16 páginasThe Zoot Suit Riothudson1963Aún no hay calificaciones
- The Number of Variants in The Greek - New TestamentDocumento16 páginasThe Number of Variants in The Greek - New Testamenthudson1963100% (1)
- The Poems of John of The Cross PDFDocumento12 páginasThe Poems of John of The Cross PDFAlleluia HaptismAún no hay calificaciones
- Earliest Gospel MenziesDocumento320 páginasEarliest Gospel Menzieshudson1963Aún no hay calificaciones
- Greek Art From Prehistoric To Classical PDFDocumento256 páginasGreek Art From Prehistoric To Classical PDFHelena AnjošAún no hay calificaciones
- Clause GPet 1Documento1 páginaClause GPet 1hudson1963Aún no hay calificaciones
- The Reception of Paul and Early Christia PDFDocumento12 páginasThe Reception of Paul and Early Christia PDFhudson1963Aún no hay calificaciones
- The Reception of Paul and Early Christia PDFDocumento12 páginasThe Reception of Paul and Early Christia PDFhudson1963Aún no hay calificaciones
- Arc-4-What S Hidd N in The HaddDocumento14 páginasArc-4-What S Hidd N in The HaddKate BrownAún no hay calificaciones
- KVUOA Toimetised 12-MännikDocumento21 páginasKVUOA Toimetised 12-MännikTalha khalidAún no hay calificaciones
- Herm Choppers PDFDocumento24 páginasHerm Choppers PDFhudson1963Aún no hay calificaciones
- Christ in Conflict An Exposition of Mark Chapter 3Documento3 páginasChrist in Conflict An Exposition of Mark Chapter 3hudson1963Aún no hay calificaciones
- BOOK REVIEW - The History of Terrorism: From Antiquity To Al Qaeda. Reviewed by Scott N. RomaniukDocumento6 páginasBOOK REVIEW - The History of Terrorism: From Antiquity To Al Qaeda. Reviewed by Scott N. Romaniukhudson1963Aún no hay calificaciones
- BOOK REVIEW - The History of Terrorism: From Antiquity To Al Qaeda. Reviewed by Scott N. RomaniukDocumento6 páginasBOOK REVIEW - The History of Terrorism: From Antiquity To Al Qaeda. Reviewed by Scott N. Romaniukhudson1963Aún no hay calificaciones
- MINIMENTAL, Puntos de Corte ColombianosDocumento5 páginasMINIMENTAL, Puntos de Corte ColombianosCatalina GutiérrezAún no hay calificaciones
- La Captura de JerusalenDocumento9 páginasLa Captura de Jerusalenhudson1963Aún no hay calificaciones
- Abraham 1Documento27 páginasAbraham 1hudson1963Aún no hay calificaciones
- The Via Moderna How Early Modern PhilosoDocumento16 páginasThe Via Moderna How Early Modern Philosohudson1963Aún no hay calificaciones
- Via ModernaDocumento24 páginasVia Modernahudson1963Aún no hay calificaciones
- The Via Moderna How Early Modern PhilosoDocumento16 páginasThe Via Moderna How Early Modern Philosohudson1963Aún no hay calificaciones
- Via ModernaDocumento24 páginasVia Modernahudson1963Aún no hay calificaciones
- QuinnHerms PDFDocumento24 páginasQuinnHerms PDFhudson1963Aún no hay calificaciones
- Nombres de Reyes MedievalesDocumento13 páginasNombres de Reyes Medievaleshudson1963Aún no hay calificaciones
- Kousser Autopsy in Athens2015Documento9 páginasKousser Autopsy in Athens2015hudson1963Aún no hay calificaciones
- The Via Moderna How Early Modern PhilosoDocumento16 páginasThe Via Moderna How Early Modern Philosohudson1963Aún no hay calificaciones
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Cerebral PalsyDocumento31 páginasCerebral PalsyYunita Amilia0% (1)
- Reflective EssayDocumento5 páginasReflective Essayjessicadietlin100% (1)
- Books and LinksDocumento3 páginasBooks and LinksLuís RochaAún no hay calificaciones
- CVPDocumento2 páginasCVPdrvcbAún no hay calificaciones
- Free Trial 28 FebDocumento1 páginaFree Trial 28 FebByron Lu Morrell0% (1)
- Fasting Glucose Insulin Ratio: A Useful Measure of Insulin Resistance in Girls With Premature AdrenarcheDocumento4 páginasFasting Glucose Insulin Ratio: A Useful Measure of Insulin Resistance in Girls With Premature AdrenarcheYOG.GANAR2291Aún no hay calificaciones
- Commentary On Spinal Stabilization Exercise.17Documento1 páginaCommentary On Spinal Stabilization Exercise.17Julenda CintarinovaAún no hay calificaciones
- Hemorragia Subaracnoidea AneurismaticaDocumento30 páginasHemorragia Subaracnoidea AneurismaticajulianaAún no hay calificaciones
- Resource - Bad Actors in Conversion Therapy PDFDocumento5 páginasResource - Bad Actors in Conversion Therapy PDFBrianna JanuaryAún no hay calificaciones
- Step On To Paediatrics 4th EditionDocumento376 páginasStep On To Paediatrics 4th EditionTawhid Zihad100% (1)
- Bullying and Ostracism Experiences in Children - JDBPDocumento9 páginasBullying and Ostracism Experiences in Children - JDBPAndreea Gligor100% (1)
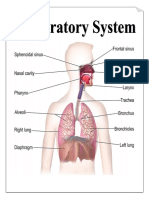
- Parts & Function of Respiratory SystemDocumento4 páginasParts & Function of Respiratory SystemLucille Ballares83% (6)
- SOP GD and Dental Specialist FINALDocumento20 páginasSOP GD and Dental Specialist FINALarpita7dr9693Aún no hay calificaciones
- Ansiedad y GastritisDocumento5 páginasAnsiedad y Gastritisjose fernandezAún no hay calificaciones
- Fa Q Internship ProgramDocumento5 páginasFa Q Internship ProgramMariam A. KarimAún no hay calificaciones
- Vicorder PWA-PWV Pres 15-04 EnglDocumento79 páginasVicorder PWA-PWV Pres 15-04 EnglHatem FaroukAún no hay calificaciones
- Medical Equipment ReplacementDocumento15 páginasMedical Equipment Replacementver_at_workAún no hay calificaciones
- Paederus Dermatitis An Outbreak On A Medical Mission AmazonDocumento3 páginasPaederus Dermatitis An Outbreak On A Medical Mission AmazonrrrawAún no hay calificaciones
- Hospital Pharmacist PDFDocumento5 páginasHospital Pharmacist PDFMuhammad YamnainAún no hay calificaciones
- Failed Spinal AnaesthesiaDocumento10 páginasFailed Spinal AnaesthesiaYosua SiwabessyAún no hay calificaciones
- Nhis Operational GuidelinesDocumento38 páginasNhis Operational GuidelinestitooluwaAún no hay calificaciones
- Systemic Vasculitis: Poonam Sharma, Mbbs Sanjeev Sharma, MD Richard Baltaro, MD and John Hurley, MDDocumento10 páginasSystemic Vasculitis: Poonam Sharma, Mbbs Sanjeev Sharma, MD Richard Baltaro, MD and John Hurley, MDHernan Del CarpioAún no hay calificaciones
- 2016 Vol 62 No - 2 - April May 2016 PDFDocumento56 páginas2016 Vol 62 No - 2 - April May 2016 PDFDanis Diba Sabatillah YaminAún no hay calificaciones
- Keratoplasty 2013.en - IdDocumento8 páginasKeratoplasty 2013.en - IdHanifiyah NabelaAún no hay calificaciones
- Pathophysiology of HyperbilirubinemiaDocumento3 páginasPathophysiology of Hyperbilirubinemiaapi-434682657Aún no hay calificaciones
- ERS Handbook For SEPAR First EditionDocumento516 páginasERS Handbook For SEPAR First Editionakanksha jha100% (2)
- List of Anesthesia Library Books PDFDocumento3 páginasList of Anesthesia Library Books PDFcommandityAún no hay calificaciones
- Historical Background of Cerebral PalsyDocumento11 páginasHistorical Background of Cerebral PalsypraveenAún no hay calificaciones
- Naturopathy: Naturopathy or Naturopathic Medicine Is A Form of AlternativeDocumento20 páginasNaturopathy: Naturopathy or Naturopathic Medicine Is A Form of AlternativeAK KJAún no hay calificaciones
- Accident Investigation ProtocolsDocumento14 páginasAccident Investigation ProtocolsgilbertwildAún no hay calificaciones