También podría gustarte
- Patho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Documento12 páginasPatho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Grant GarcesAún no hay calificaciones
- Pediatric Cardiology II Lecture SummaryDocumento5 páginasPediatric Cardiology II Lecture SummaryMedisina101Aún no hay calificaciones
- PyodermaDocumento19 páginasPyodermaFajar Hidayat RamadhanAún no hay calificaciones
- The Luo-Connecting Deadman ArticlDocumento7 páginasThe Luo-Connecting Deadman ArticlavaAún no hay calificaciones
- Abdominal Trauma Signs, Symptoms and Nursing CareDocumento24 páginasAbdominal Trauma Signs, Symptoms and Nursing CareSurgeryClassesAún no hay calificaciones
- Upper Gastrointestinal Bleeding (Ugib) : First Shift: August 13, 2018Documento10 páginasUpper Gastrointestinal Bleeding (Ugib) : First Shift: August 13, 2018Angelo Dela Cruz VillaromanAún no hay calificaciones
- Medicine 6.1b Approach To Cancer Patients - FernandoDocumento7 páginasMedicine 6.1b Approach To Cancer Patients - FernandoAbigail LausAún no hay calificaciones
- History Taking PancreatitisDocumento11 páginasHistory Taking PancreatitisToria053100% (1)
- Pharmacology of EthanolDocumento5 páginasPharmacology of EthanolJoshua RemonAún no hay calificaciones
- Cervical Cancer Screening and TreatmentDocumento104 páginasCervical Cancer Screening and TreatmentArie PratamaAún no hay calificaciones
- Pediatric ProblemsDocumento4 páginasPediatric ProblemsRencel Hope Bañez100% (1)
- Anatomy of the SpleenDocumento18 páginasAnatomy of the Spleenزين العابدين محمد عويش100% (1)
- Evaluation of Abdominal PainDocumento7 páginasEvaluation of Abdominal PainCherry Faith Merisco LabtangAún no hay calificaciones
- Esophageal Achalasia DysphagiaDocumento14 páginasEsophageal Achalasia DysphagiaTirtha Taposh100% (1)
- Acute Gastroenteritis in Children: Prepared By: Prof. Elizabeth D. Cruz RN, ManDocumento12 páginasAcute Gastroenteritis in Children: Prepared By: Prof. Elizabeth D. Cruz RN, ManChaii De GuzmanAún no hay calificaciones
- Fluids and Electrolytes Management in Surgical PatientsDocumento4 páginasFluids and Electrolytes Management in Surgical PatientsJanine Maita BalicaoAún no hay calificaciones
- 1 LiverDocumento10 páginas1 LiverAlbino Fulgencio Santos III100% (1)
- Pediatrics SamplexDocumento6 páginasPediatrics SamplexThea SansonAún no hay calificaciones
- Peptic Ulcer DiseaseDocumento14 páginasPeptic Ulcer DiseasePernel Jose Alam MicuboAún no hay calificaciones
- DISC, Drugs, Infection, Thick Basal MembraneDocumento5 páginasDISC, Drugs, Infection, Thick Basal MembraneHOPEAún no hay calificaciones
- 3 Surgery - Mediastinum and PleuraDocumento6 páginas3 Surgery - Mediastinum and PleuraCassey Koi FarmAún no hay calificaciones
- Headache History: Introduction - WIPPPDocumento4 páginasHeadache History: Introduction - WIPPPAmjad_2020Aún no hay calificaciones
- UROLOGY 2020 (Doc BarcenasDocumento33 páginasUROLOGY 2020 (Doc BarcenasJüdith Marie Reyes BauntoAún no hay calificaciones
- Acute Poststreptococcal GlomerulonephritisDocumento69 páginasAcute Poststreptococcal GlomerulonephritisJirran CabatinganAún no hay calificaciones
- IM - Cardiomyopathy and MyocarditisDocumento9 páginasIM - Cardiomyopathy and MyocarditisElisha BernabeAún no hay calificaciones
- IKD9 - Radiological Evaluation of Renal CystsDocumento26 páginasIKD9 - Radiological Evaluation of Renal CystsRenal Association MauritiusAún no hay calificaciones
- RabiesDocumento10 páginasRabiesWinda LiraAún no hay calificaciones
- Blood Supply of HeartDocumento7 páginasBlood Supply of Heartmariposa_0612Aún no hay calificaciones
- Etiology and Diagnosis of Bile Duct StonesDocumento8 páginasEtiology and Diagnosis of Bile Duct Stoneskuncupcupu1368Aún no hay calificaciones
- Joint Pain - ApproachDocumento32 páginasJoint Pain - ApproachHassan Bin AjmalAún no hay calificaciones
- Case 1 History & PEDocumento3 páginasCase 1 History & PEcbac1990Aún no hay calificaciones
- HyphemaDocumento19 páginasHyphemaLiyanti RinceAún no hay calificaciones
- Malignant Neoplasm (Ovarian Cancer)Documento4 páginasMalignant Neoplasm (Ovarian Cancer)nursing concept mapsAún no hay calificaciones
- Clinical Management: PGI Eileen Andres PediatricsDocumento9 páginasClinical Management: PGI Eileen Andres PediatricsMichael BonillaAún no hay calificaciones
- Surgical Oncology and Breast BiopsyDocumento12 páginasSurgical Oncology and Breast Biopsybo gum parkAún no hay calificaciones
- Belle Cervical DiseaseDocumento7 páginasBelle Cervical DiseaseRashed ShatnawiAún no hay calificaciones
- Acute PancreatitisDocumento4 páginasAcute PancreatitisKEn PilapilAún no hay calificaciones
- Examination of Breast Lump PDFDocumento2 páginasExamination of Breast Lump PDFDanaAún no hay calificaciones
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocumento4 páginasNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedAún no hay calificaciones
- Sheehan SyndromeDocumento6 páginasSheehan SyndromeArvie TagnongAún no hay calificaciones
- Pre-Res Case Presentation: Jo Anne N. Ramos, MDDocumento72 páginasPre-Res Case Presentation: Jo Anne N. Ramos, MDKah Mote KyuAún no hay calificaciones
- MED - Finals 1.5 - Asthma PDFDocumento12 páginasMED - Finals 1.5 - Asthma PDFYestin Reece Corpus ArcegaAún no hay calificaciones
- Bacterial MeningitisDocumento1 páginaBacterial MeningitisDavid HylandAún no hay calificaciones
- Pancreatic Cancer (Cancer of The Pancreas) : Patient Discussions: FindDocumento13 páginasPancreatic Cancer (Cancer of The Pancreas) : Patient Discussions: FindMoses ZainaAún no hay calificaciones
- Kelenjar LakrimalDocumento44 páginasKelenjar LakrimalNurfanida Natasya MAún no hay calificaciones
- ACUTE GASTROENTERITIS GUIDEDocumento54 páginasACUTE GASTROENTERITIS GUIDEVincent LaranjoAún no hay calificaciones
- Total Abdominal HysterectomyDocumento19 páginasTotal Abdominal HysterectomyMeidina Rachma Amanda100% (1)
- Cough: PHR Sangita ShakyaDocumento21 páginasCough: PHR Sangita ShakyaCurex QAAún no hay calificaciones
- Infectious Disease GuideDocumento33 páginasInfectious Disease GuideSilvia KesegAún no hay calificaciones
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocumento27 páginasHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanAún no hay calificaciones
- Pancreatic AdenocarcinomaDocumento6 páginasPancreatic AdenocarcinomafikriafisAún no hay calificaciones
- Tourniquet Test: Small Amount of Air Will Not Harm The TissuesDocumento4 páginasTourniquet Test: Small Amount of Air Will Not Harm The TissuesjoymaeannAún no hay calificaciones
- Peripheral Vascular Disease-1Documento52 páginasPeripheral Vascular Disease-1Johiarra Madanglog Tabigne100% (1)
- Management of Acute Appendicitis in Adults - UpToDateDocumento28 páginasManagement of Acute Appendicitis in Adults - UpToDateVinicius VieiraAún no hay calificaciones
- Thermal InjuryDocumento35 páginasThermal InjuryIbrahim SalimAún no hay calificaciones
- Congestive Heart FailureDocumento24 páginasCongestive Heart FailureKoka KolaAún no hay calificaciones
- PyelonephritisDocumento17 páginasPyelonephritisapi-339668544100% (1)
- 5.4 IHD HHD CHF Cor PulmonaleDocumento15 páginas5.4 IHD HHD CHF Cor PulmonaleMemay velascoAún no hay calificaciones
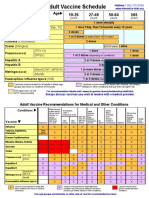
- Adult Vaccine Schedule Eng PDFDocumento2 páginasAdult Vaccine Schedule Eng PDFAbdur RehmanAún no hay calificaciones
- PEDIA2 - 4-3 Congenital Heart DiseasesDocumento19 páginasPEDIA2 - 4-3 Congenital Heart DiseasesRadha ChiombonAún no hay calificaciones
- Pharmacology Table - GonzalesDocumento14 páginasPharmacology Table - GonzalesMark Angelo PonferradoAún no hay calificaciones
- Preoperative Care Guide for SurgeonsDocumento33 páginasPreoperative Care Guide for SurgeonsPrincewill SeiyefaAún no hay calificaciones
- Problem-based Approach to Gastroenterology and HepatologyDe EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisAún no hay calificaciones
- Infective Endocarditis - Dr. Payawal PDFDocumento6 páginasInfective Endocarditis - Dr. Payawal PDFMedisina101Aún no hay calificaciones
- Diagnosing Chest Pain CausesDocumento8 páginasDiagnosing Chest Pain CausesMedisina101Aún no hay calificaciones
- Congestive Heart Failure - Dra. DeduyoDocumento10 páginasCongestive Heart Failure - Dra. DeduyoMedisina101Aún no hay calificaciones
- Acute Coronary Syndrome - Dra. Deduyo PDFDocumento6 páginasAcute Coronary Syndrome - Dra. Deduyo PDFMedisina101Aún no hay calificaciones
- Cardiac Tumors - Dr. BartolomeDocumento12 páginasCardiac Tumors - Dr. BartolomeMedisina101Aún no hay calificaciones
- Diseases of the Aorta: Causes and Types of Aortic AneurysmsDocumento11 páginasDiseases of the Aorta: Causes and Types of Aortic AneurysmsMedisina101Aún no hay calificaciones
- ECG Part 1 - Dr. Payawal PDFDocumento10 páginasECG Part 1 - Dr. Payawal PDFMedisina101Aún no hay calificaciones
- Coronary Artery Disease - Dra. Deduyo PDFDocumento7 páginasCoronary Artery Disease - Dra. Deduyo PDFMedisina101Aún no hay calificaciones
- Detecting Abnormal Cardiac RhythmsDocumento10 páginasDetecting Abnormal Cardiac RhythmsMedisina101100% (1)
- Peripheral Vascular Medicine - Dr. Deduyo PDFDocumento14 páginasPeripheral Vascular Medicine - Dr. Deduyo PDFMedisina101Aún no hay calificaciones
- Arrythmia Part 2 - Dr. Payawal PDFDocumento8 páginasArrythmia Part 2 - Dr. Payawal PDFMedisina101Aún no hay calificaciones
- Pedia Pulmo 3 11.03.16Documento49 páginasPedia Pulmo 3 11.03.16Medisina101Aún no hay calificaciones
- ECG Part 2 - Dr. Payawal PDFDocumento4 páginasECG Part 2 - Dr. Payawal PDFMedisina101Aún no hay calificaciones
- Deep Vein Thrombosis - Dr. Deduyo PDFDocumento17 páginasDeep Vein Thrombosis - Dr. Deduyo PDFMedisina101Aún no hay calificaciones
- Valvular Heart Diseases Part 1 - Dr. BartolomeDocumento18 páginasValvular Heart Diseases Part 1 - Dr. BartolomeMedisina101Aún no hay calificaciones
- Congenital Heart Diseases - Dr. BartolomeDocumento12 páginasCongenital Heart Diseases - Dr. BartolomeMedisina101Aún no hay calificaciones
- PEDIA - Cardio (Esguerra) PDFDocumento9 páginasPEDIA - Cardio (Esguerra) PDFMedisina101Aún no hay calificaciones
- Pedia Pulmo I 10.4.16Documento129 páginasPedia Pulmo I 10.4.16Medisina101Aún no hay calificaciones
- Pedia Pulmo 2 10.18.16Documento73 páginasPedia Pulmo 2 10.18.16Medisina101Aún no hay calificaciones
- Cardiac Tumors Slides - Dr. BartolomeDocumento81 páginasCardiac Tumors Slides - Dr. BartolomeMedisina101Aún no hay calificaciones
- Acquired Heart DiseaseDocumento44 páginasAcquired Heart DiseaseMedisina101Aún no hay calificaciones
- SURGERY Lecture 5 - Abdominal Wall, Omentum, Mesentery, Retroperitoneum (Dr. Wenceslao)Documento13 páginasSURGERY Lecture 5 - Abdominal Wall, Omentum, Mesentery, Retroperitoneum (Dr. Wenceslao)Medisina101Aún no hay calificaciones
- SURGERY Lecture 4 - Breast (Dra. Fernandez)Documento15 páginasSURGERY Lecture 4 - Breast (Dra. Fernandez)Medisina101100% (1)
- External Abdominal Hernias GuideDocumento12 páginasExternal Abdominal Hernias GuideMedisina101100% (1)
- SURGERY Lecture 2 - Liver & Gallbladder (Dr. Wenceslao)Documento19 páginasSURGERY Lecture 2 - Liver & Gallbladder (Dr. Wenceslao)Medisina101100% (1)
- SURGERY Lecture 1 - Small Intestine (Dr. Mendoza)Documento16 páginasSURGERY Lecture 1 - Small Intestine (Dr. Mendoza)Medisina101100% (1)
- Head and Neck SurgeryDocumento15 páginasHead and Neck SurgeryMedisina101100% (1)
- Surgery II - Pancreas 2014Documento20 páginasSurgery II - Pancreas 2014Medisina101Aún no hay calificaciones
- Deep neck infections guideDocumento16 páginasDeep neck infections guideSiska HarapanAún no hay calificaciones
- Hand Washing Basics To Help Your Family Stay SafeDocumento4 páginasHand Washing Basics To Help Your Family Stay Safechandy Rendaje100% (1)
- Pathology of Female Genital Tract Short NotesDocumento5 páginasPathology of Female Genital Tract Short NotesameerabestAún no hay calificaciones
- Home Visit Nursing CareDocumento28 páginasHome Visit Nursing CareSaad AlkhathamiAún no hay calificaciones
- Grama PriyaDocumento5 páginasGrama PriyaRajesh RaiAún no hay calificaciones
- Infective Endocarditis: Diagnosis and ManagementDocumento26 páginasInfective Endocarditis: Diagnosis and Managementrameshbmc100% (1)
- Small Pox: A Child Infected With SmallpoxDocumento5 páginasSmall Pox: A Child Infected With SmallpoxJavee_Viccent__5618Aún no hay calificaciones
- Maternal and Newborn Nursing AbbreviationsDocumento3 páginasMaternal and Newborn Nursing AbbreviationsjamesAún no hay calificaciones
- 500-ALPHA FIT Testers ManualDocumento29 páginas500-ALPHA FIT Testers ManualDarío Gerpe MeirásAún no hay calificaciones
- SIR Epidemic Model Explained: Susceptible, Infected, Recovered PopulationsDocumento16 páginasSIR Epidemic Model Explained: Susceptible, Infected, Recovered Populationsmirast91Aún no hay calificaciones
- Cerebral PalsyDocumento55 páginasCerebral PalsyFuküi AliAún no hay calificaciones
- Borang Mohon VisaDocumento4 páginasBorang Mohon Visanadirah400Aún no hay calificaciones
- 01 - Introduction To DentistryDocumento18 páginas01 - Introduction To Dentistrymichal ben meronAún no hay calificaciones
- Document WPS OfficeDocumento3 páginasDocument WPS OfficeWenalyn Grace Abella LlavanAún no hay calificaciones
- Case Study ChipotleDocumento3 páginasCase Study Chipotleapi-288102944Aún no hay calificaciones
- Vaginal Discharge Flow ChartDocumento1 páginaVaginal Discharge Flow ChartHafizuddin RazidAún no hay calificaciones
- SANITIZING TUNNEL PPT FinalDocumento12 páginasSANITIZING TUNNEL PPT FinalSOUMYA HAún no hay calificaciones
- 01 Body Conformation of HorseDocumento32 páginas01 Body Conformation of HorseDrSagar Mahesh Sonwane100% (3)
- 2 Tema History of MedicineDocumento6 páginas2 Tema History of MedicineUgnė TurauskaitėAún no hay calificaciones
- Idiopathic Calcinosis Cutis of ScrotumDocumento4 páginasIdiopathic Calcinosis Cutis of ScrotumEtty FaridaAún no hay calificaciones
- List of Phobias and Simple Cures PDFDocumento40 páginasList of Phobias and Simple Cures PDFAnu KumarAún no hay calificaciones
- Idcases: Stephanie Stephanie, Sarah A. SchmalzleDocumento3 páginasIdcases: Stephanie Stephanie, Sarah A. SchmalzlearturomarticarvajalAún no hay calificaciones
- Creation of School Task Force Covid: Schools Division Office of PampangaDocumento1 páginaCreation of School Task Force Covid: Schools Division Office of PampangaRames Ely GJ100% (1)
- Nestle Controversial IssuesDocumento2 páginasNestle Controversial IssuesTatadarz Auxtero LagriaAún no hay calificaciones
- Perio Clinic ManualDocumento48 páginasPerio Clinic ManualPetia TerzievaAún no hay calificaciones
- Herpes LabialisDocumento3 páginasHerpes LabialisSuganya MurugaiahAún no hay calificaciones
- The Evaluation of Food Hygiene Knowledge, Attitudes, and PracticesDocumento6 páginasThe Evaluation of Food Hygiene Knowledge, Attitudes, and PracticessyooloveAún no hay calificaciones
- Cubital Tunnel SyndromeDocumento1 páginaCubital Tunnel SyndromeIlhamDevirxaAún no hay calificaciones