Documentos de Académico
Documentos de Profesional
Documentos de Cultura
Risk of A Thrombotic Event After The 6-Week Postpartum Period
Cargado por
CintyaRolitaTítulo original
Derechos de autor
Formatos disponibles
Compartir este documento
Compartir o incrustar documentos
¿Le pareció útil este documento?
¿Este contenido es inapropiado?
Denunciar este documentoCopyright:
Formatos disponibles
Risk of A Thrombotic Event After The 6-Week Postpartum Period
Cargado por
CintyaRolitaCopyright:
Formatos disponibles
The n e w e ng l a n d j o u r na l of m e dic i n e
original article
Risk of a Thrombotic Event
after the 6-Week Postpartum Period
Hooman Kamel, M.D., Babak B. Navi, M.D., Nandita Sriram, B.S.,
Dominic A. Hovsepian, B.S., Richard B. Devereux, M.D.,
and Mitchell S.V. Elkind, M.D.
A BS T R AC T
Background
The postpartum state is associated with a substantially increased risk of thrombo- From the Department of Neurology (H.K.,
sis. It is uncertain to what extent this heightened risk persists beyond the conven- B.B.N., N.S., D.A.H.), Feil Family Brain
and Mind Research Institute (H.K., B.B.N.),
tionally defined 6-week postpartum period. and Division of Cardiology (R.B.D.), Weill
Cornell Medical College, the Department
Methods of Neurology, Columbia College of Physi
cians and Surgeons (M.S.V.E.), and the
Using claims data on all discharges from nonfederal emergency departments and Department of Epidemiology, Mailman
acute care hospitals in California, we identified women who were hospitalized for School of Public Health, Columbia Uni
labor and delivery between January 1, 2005, and June 30, 2010. We used validated versity (M.S.V.E.) all in New York.
Address reprint requests to Dr. Kamel at
diagnosis codes to identify a composite primary outcome of ischemic stroke, acute 407 E. 61st St., 5th Fl., New York, NY 10065,
myocardial infarction, or venous thromboembolism. We then used conditional logis- or at hok9010@med.cornell.edu.
tic regression to assess each patients likelihood of a first thrombotic event during
This article was published on February 13,
sequential 6-week periods after delivery, as compared with the corresponding 2014, at NEJM.org.
6-week period 1 year later.
N Engl J Med 2014;370:1307-15.
DOI: 10.1056/NEJMoa1311485
Results Copyright 2014 Massachusetts Medical Society.
Among the 1,687,930 women with a first recorded delivery, 1015 had a thrombotic
event (248 cases of stroke, 47 cases of myocardial infarction, and 720 cases of ve-
nous thromboembolism) in the period of 1 year plus up to 24 weeks after delivery.
The risk of primary thrombotic events was markedly higher within 6 weeks after
delivery than in the same period 1 year later, with 411 events versus 38 events, for an
absolute risk difference of 22.1 events (95% confidence interval [CI], 19.6 to 24.6)
per 100,000 deliveries and an odds ratio of 10.8 (95% CI, 7.8 to 15.1). There was also
a modest but significant increase in risk during the period of 7 to 12 weeks after
delivery as compared with the same period 1 year later, with 95 versus 44 events,
for an absolute risk difference of 3.0 events (95% CI, 1.6 to 4.5) per 100,000 deliver-
ies and an odds ratio of 2.2 (95% CI, 1.5 to 3.1). Risks of thrombotic events were
not significantly increased beyond the first 12 weeks after delivery.
Conclusions
Among patients in our study, an elevated risk of thrombosis persisted until at least
12 weeks after delivery. However, the absolute increase in risk beyond 6 weeks after
delivery was low. (Funded by the National Institute of Neurological Disorders and
Stroke.)
n engl j med 370;14nejm.orgapril 3, 2014 1307
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
P
regnancy significantly increases and Development.15 After a multistep quality-as-
the risk of thrombosis. This heightened surance process to flag invalid or inconsistent
thrombotic risk rises further during the entries, these data were provided in a deidenti-
postpartum period, which is conventionally de- fied format to the Healthcare Cost and Utilization
fined as the 6 weeks after delivery.1 As compared Project.14 The institutional review boards at
with the nonpregnant state, the 6-week postpar- Weill Cornell Medical College and Columbia
tum period is associated with increases by a factor University Medical Center certified that this
of 3 to 9 in the risk of stroke, by a factor of 3 to analysis of publicly available, deidentified data
6 in the risk of myocardial infarction, and by a was exempt from review and from the need for
factor of 9 to 22 in the risk of venous thrombo- informed consent. All authors take responsibility
embolism.2-8 It is unknown whether these risks for the integrity of the data and analyses.
remain increased after the conventionally de-
fined 6-week postpartum period. Guidelines for Study Patients
the treatment of thrombotic disorders during We identified all women who had been hospital-
pregnancy advise the discontinuation of prophy- ized for labor and delivery, using standard codes
lactic therapy at 6 weeks after delivery in women from the International Classification of Diseases, 9th
at high risk for venous thromboembolism.1 How- Revision, Clinical Modification (ICD-9-CM) for vag-
ever, previous studies and isolated case reports inal delivery (72, 73, 75, V27, or 650659) and
have suggested that an increased thrombotic risk cesarean delivery (74).16 To maximize longitudi-
may persist beyond 6 weeks after delivery.5,8-10 nal follow-up, we excluded non-California resi-
Therefore, more data are needed to rigorously as- dents. We included patients 12 years of age or
sess the risk after the 6-week postpartum period. older, given the infrequency of births among pa-
We designed this study to assess the duration of tients younger than 12 years of age (<0.1% of all
an increased postpartum thrombotic risk in a births17). Post hoc sensitivity analyses that in-
large population-based cohort of women. cluded patients regardless of age or included only
patients 18 years of age or older did not substan-
Me thods tially alter our findings.
For women with multiple labor-related hospi-
Study Design talizations during a single 40-week period, we
We performed a retrospective crossover-cohort excluded cases of false labor by identifying deliv-
study (a study design in which each patient serves ery as the latest hospitalization during that time.
as his or her own control), using administrative Since women who have had a thrombotic event
claims data on all discharges from nonfederal may be less likely to subsequently become preg-
emergency departments and acute care hospitals nant, we included only the first pregnancy cap-
in California. We compared each patients likeli- tured in our database for each patient. To focus
hood of a first thrombotic event during sequen- on incident outcomes, we excluded patients who
tial 6-week periods after delivery with the likeli- had had any thrombosis diagnoses before their
hood of an event during the corresponding first recorded delivery (see the Methods section
6-week period 1 year later. Since exposure to in the Supplementary Appendix, available with
pregnancy varies discretely over time, this design the full text of this article at NEJM.org, for defi-
allowed each patient to serve as her own control, nitions).
thereby minimizing unmeasured confounding.11,12 To compare thrombotic risk during the post-
California was chosen because it is a large and partum period with the risk during nonpregnant
demographically heterogeneous state13 with ad- periods, we excluded patients with a second de-
ministrative data that allow tracking of individu- livery during the follow-up period. We included
al patients across visits over numerous years,14 hospitalizations for labor starting on January 1,
thereby providing sufficient statistical power to 2005, when patient-specific longitudinal tracking
detect associations among conditions with low identifiers were introduced in these databases.14
absolute event rates. Analysts at each facility Data were available through December 31, 2011,14
used detailed reporting and formatting specifi- so to accommodate analyses of the 24 weeks
cations and automated online-reporting software after delivery and the same 24-week period 1 year
to provide uniform data on all discharges to the later, we included patients with a hospitalization
California Office of Statewide Health Planning for a first labor through June 30, 2010.
1308 n engl j med 370;14nejm.orgapril 3, 2014
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
Thrombotic Risk after 6-Week Postpartum Period
Study Outcomes and Measurements would progressively decrease across sequential
The primary outcome was a composite of ische 6-week periods but remain significantly elevated
mic stroke, acute myocardial infarction, or ve- at least through the period of 7 to 12 weeks after
nous thromboembolism. We identified these delivery. To help ensure that visits that were relat-
outcomes using validated diagnosis-code algo- ed to venous thromboembolism did not represent
rithms that were previously shown to have a pos- the sequelae of previous outpatient diagnoses,
itive predictive value of 90% or more (see the we performed a sensitivity analysis that excluded
Supplementary Appendix).18-20 To maximize ac- diagnoses of venous thromboembolism with a
curacy, we limited our case ascertainment to concomitant bleeding-related diagnosis,24 since
stroke and myocardial infarction resulting in the event may have represented a complication of
hospitalization but included discharges from the preexisting anticoagulant therapy.
emergency department as well as hospitalizations To assess the sensitivity of our results to our
for venous thromboembolism, since this condi- baseline model structure, we inverted the model
tion is now often managed in the outpatient set- and performed a case-crossover analysis. We
ting.21 To focus on incident outcomes and avoid identified all women who were 12 years of age
bias from the effects of antithrombotic therapy or older in whom the primary outcome had been
prescribed after the initial thrombotic event, we diagnosed from July 1, 2006, to December 31,
included a maximum of one thrombosis diagno- 2011. We compared the likelihood of a first re-
sis for each patient; however, in a sensitivity corded labor and delivery during days 0 through
analysis, we also included thrombosis diagnoses 41 before the thrombotic event versus the same
subsequent to the index event. 6-week period exactly 1 year earlier. We repeated
In addition to the primary composite outcome, this case-crossover analysis for postpartum days
we separately assessed arterial events (stroke or 42 to 83, 84 to 125, and 126 to 167 before the
myocardial infarction) as compared with venous thrombotic event. In a sensitivity analysis, we in-
thromboembolism. The definition of venous cluded only cases that occurred beyond 1 year
thromboembolism in our primary analysis did 24 weeks after a first documented delivery. This
not include cerebral venous thrombosis because nested design ensured that all patients were alive
that condition lacks rigorously validated ICD-9- and under observation throughout the entire
CM diagnosis codes, but it was included among study period, while also allowing us to assess
secondary outcomes, which consisted of the pri- the effects of the inclusion of pregnancies sub-
mary outcome plus a broader set of other throm- sequent to the first.
bosis diagnoses (see the Supplementary Appendix We performed a separate post hoc casecon-
for definitions). trol analysis to confirm whether any heightened
We performed subgroup analyses stratified risk of postpartum thrombosis was associated
according to thrombotic risk, using ICD-9-CM with labor and delivery specifically, rather than
codes to identify consistently reported risk fac- with hospitalization in general. We defined cases
tors for postpartum thrombosis: maternal age of and controls on the basis of the presence or ab-
more than 35 years, primary hypercoagulable sence of the primary outcome. The exposure vari-
state, eclampsia or preeclampsia, smoking, and able was a preceding hospitalization for delivery
cesarean delivery (see the Supplementary Appen versus for any other diagnosis. To account for
dix for definitions).1,3,22,23 potential confounders, these analyses were ad-
justed for age, race, insurance type, the presence
Statistical Analysis or absence of a primary hypercoagulable state,
For each patient, we compared the likelihood of smoking, and the Elixhauser comorbidity index.25
a first-ever recorded thrombosis during postpar-
tum days 0 through 41 versus the same period R e sult s
exactly 1 year later. We repeated this crossover-
cohort analysis for postpartum days 42 through Study Population
83, 84 through 125, and 126 through 167. We We identified 1,687,930 California residents with
used conditional logistic regression to calculate a first recorded hospitalization for labor and de-
odds ratios for each interval because each patient livery between January 1, 2005, and June 30, 2010.
was matched to her own crossover period 1 year This number was within 6% of the expected
later.11 Our a priori hypothesis was that the risk number on the basis of birth certificates issued
n engl j med 370;14nejm.orgapril 3, 2014 1309
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
during that time.17 In the 1 year 24 weeks after per 100,000 deliveries), corresponding to an ab-
delivery, 1015 women had a thrombotic event solute risk difference of 22.1 (95% confidence
(248 cases of stroke, 47 cases of myocardial in- interval [CI], 19.6 to 24.6) per 100,000 deliveries
farction, and 720 cases of venous thromboembo- and an odds ratio of 10.8 (95% CI, 7.8 to 15.1). In
lism). As compared with patients without post- the period of 7 to 12 weeks after delivery, there
partum thrombosis, those with postpartum was a modest but still significant increase in the
thrombotic events were older, were more likely to number of thrombotic events, as compared with
be white or black than Hispanic or Asian, were the same period 1 year later (95 events, or 5.6 events
less often privately insured, and were more likely per 100,000 deliveries, vs. 44 events, or 2.6 events
to have risk factors for thrombosis (Table 1). per 100,000 deliveries), corresponding to an ab-
solute risk difference of 3.0 (95% CI, 1.6 to 4.5)
Risk of Thrombotic Events per 100,000 deliveries and an odds ratio of 2.2
Significantly more thrombotic events occurred (95% CI, 1.5 to 3.1).
within 6 weeks after delivery than during the The risk was no longer significantly elevated
same period 1 year later (411 events, or 24.4 events after 12 weeks, with an odds ratio of 1.4 (95% CI,
per 100,000 deliveries, vs. 38 events, or 2.3 events 0.9 to 2.1) for the period of 13 to 18 weeks after
delivery and an odds ratio of 1.0 (95% CI, 0.7 to
Table 1. Baseline Characteristics of the Patients, According to the Presence 1.4) for the period of 19 to 24 weeks after deliv-
or Absence of a Postpartum Thrombotic Event.*
ery (Table 2). In post hoc exploratory analyses,
Thrombotic No Thrombotic the thrombotic risk was increased during the
Event Event period of 13 to 15 weeks after delivery (odds
Characteristic (N=1015) (N=1,686,915)
ratio, 2.0; 95% CI, 1.1 to 3.6) but was no longer
Age yr 29.57.2 28.06.7 elevated in the period of 16 to 18 weeks (odds
Race or ethnic group no. (%) ratio, 1.0; 95% CI, 0.6 to 1.8) (Fig. 1, and Table
White 430 (42.4) 635,852 (37.7) S1 in the Supplementary Appendix).
Black 135 (13.3) 99,486 (5.9) The risk of thrombosis during the period of
Hispanic 293 (28.9) 593,790 (35.2) 7 to 12 weeks after delivery appeared to be
similarly elevated for arterial events (odds ratio,
Asian or Pacific Islander 66 (6.5) 188,125 (11.2)
2.1; 95% CI, 1.0 to 4.3) and venous events (odds
Native American 2 (0.2) 2,208 (0.1)
ratio, 2.2; 95% CI, 1.4 to 3.3), although the abso-
Other 24 (2.4) 49,024 (2.9) lute risk difference was especially low for arterial
Missing data 65 (6.4) 118,430 (7.0) events. We found a similar temporal pattern of
Payment source no. (%) thrombotic risk in the secondary analysis, which
Medicare 9 (0.9) 6,764 (0.4) included a broader set of thrombosis diagnoses,
Medicaid 344 (33.9) 500,534 (29.7)
including cerebral venous thrombosis (Table 2).
The period during which thrombotic risk was
Private insurance 516 (50.8) 1,021,579 (60.6)
significantly increased was also materially un-
Self-pay 93 (9.2) 104,111 (6.2)
changed in sensitivity analyses that excluded
Other 53 (5.2) 53,526 (3.2) diagnoses of venous thromboembolism with
Missing data 0 401 (<0.1) accompanying bleeding codes or that included
Thrombotic risk factors no. (%) thrombosis diagnoses subsequent to the first
Age >35 yr 264 (26.0) 271,729 (16.1) recorded event. Except for a significantly higher
Eclampsia or preeclampsia 240 (23.6) 131,527 (7.8)
risk within 6 weeks after delivery among women
who had undergone cesarean section than among
Primary hypercoagulable state 8 (0.8) 1,495 (0.1)
those who had undergone vaginal delivery, we
Smoking 45 (4.4) 29,853 (1.8) found no significant variation in thrombotic risk
Cesarean delivery 490 (48.3) 548,217 (32.5) over the different time periods across subgroups
with or without thrombotic risk factors (Tables
* Plusminus values are means SD. Between-group differences for all baseline
characteristics were significant (P<0.001). Percentages may not total 100 be S2 and S3 in the Supplementary Appendix).
cause of rounding.
Race or ethnic group was reported by patients or their surrogates. Case-Crossover and CaseControl Analyses
Primary hypercoagulable state was defined according to diagnosis code 289.81
in the International Classification of Diseases, 9th Revision, Clinical Modification. In a case-crossover analysis of the likelihood of
labor and delivery before a first thrombotic event
1310 n engl j med 370;14nejm.orgapril 3, 2014
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
Thrombotic Risk after 6-Week Postpartum Period
Table 2. Number and Rate of Postpartum Thrombotic Events during Sequential 6-Week Intervals after Labor and Delivery.*
Time Interval after Labor Case Crossover Absolute Risk Difference Odds Ratio
and Delivery and Outcome Period Period (95% CI) (95% CI)
no. of events (rate per
100,000 deliveries)
Weeks 06
Stroke, myocardial infarction, or 411 (24.4) 38 (2.3) 22.1 (19.6 to 24.6) 10.8 (7.8 to 15.1)
venous thromboembolism
Stroke 119 (7.1) 14 (0.8) 6.2 (4.8 to 7.6) 8.5 (4.9 to 14.8)
Myocardial infarction 13 (0.8) 1 (0.1) 0.7 (0.2 to 1.2) 13.0 (1.7 to 99.4)
Venous thromboembolism 279 (16.5) 23 (1.4) 15.2 (13.1 to 17.2) 12.1 (7.9 to 18.6)
Stroke, myocardial infarction, venous 2253 (133.5) 99 (5.9) 127.6 (121.9 to 133.3) 22.8 (18.6 to 27.8)
thromboembolism, or other
Weeks 712
Stroke, myocardial infarction, or 95 (5.6) 44 (2.6) 3.0 (1.6 to 4.5) 2.2 (1.5 to 3.1)
venous thromboembolism
Stroke 15 (0.9) 9 (0.5) 0.4 (0.3 to 1.0) 1.7 (0.7 to 3.8)
Myocardial infarction 8 (0.5) 2 (0.1) 0.4 (0.1 to 0.8) 4.0 (0.8 to 18.8)
Venous thromboembolism 72 (4.3) 33 (2.0) 2.3 (1.1 to 3.6) 2.2 (1.4 to 3.3)
Stroke, myocardial infarction, venous 197 (11.7) 94 (5.6) 6.1 (4.1 to 8.1) 2.1 (1.6 to 2.7)
thromboembolism, or other
Weeks 1318
Stroke, myocardial infarction, or 55 (3.3) 39 (2.3) 0.9 (0.2 to 2.1) 1.4 (0.9 to 2.1)
venous thromboembolism
Stroke 9 (0.5) 9 (0.5) 0 (0.6 to 0.6) 1.0 (0.4 to 2.5)
Myocardial infarction 2 (0.1) 2 (0.1) 0 (0.3 to 0.3) 1.0 (0.1 to 7.1)
Venous thromboembolism 44 (2.6) 28 (1.7) 0.9 (0.1 to 2.0) 1.6 (1.0 to 2.5)
Stroke, myocardial infarction, venous 99 (5.9) 95 (5.6) 0.2 (1.4 to 1.9) 1.0 (0.8 to 1.4)
thromboembolism, or other
Weeks 1924
Stroke, myocardial infarction, or 52 (3.1) 53 (3.1) 0.1 (1.3 to 1.2) 1.0 (0.7 to 1.4)
venous thromboembolism
Stroke 16 (0.9) 15 (0.9) 0.1 (0.6 to 0.8) 1.1 (0.5 to 2.2)
Myocardial infarction 5 (0.3) 2 (0.1) 0.2 (0.2 to 0.5) 2.5 (0.5 to 12.9)
Venous thromboembolism 31 (1.8) 36 (2.1) 0.3 (1.3 to 0.7) 0.9 (0.5 to 1.4)
Stroke, myocardial infarction, venous 98 (5.8) 113 (6.7) 0.9 (2.6 to 0.9) 0.9 (0.7 to 1.1)
thromboembolism, or other
* Data for the case period are for the indicated interval after labor and delivery. Data for the crossover period are for the
indicated interval plus 1 year after labor and delivery. Discrepancies between the reported risks for individual and com
posite end points or for different periods are due to rounding.
Listed are the absolute differences in rate per 100,000 deliveries between the case period and the crossover period.
Odds ratios are for the case period versus the crossover period, as calculated with the use of conditional logistic re
gression.
The composite of ischemic stroke, acute myocardial infarction, or venous thromboembolism was the primary outcome.
The secondary outcome consisted of the primary outcome plus a broader set of thrombosis diagnoses, including cere
bral venous thrombosis (see the Methods section in the Supplementary Appendix for diagnosis definitions).
versus the same periods 1 year earlier, we found 13.9), significantly elevated in the period of 7 to
that the odds of a first delivery were markedly 12 weeks before a thrombotic event (odds ratio,
elevated in the period of 0 to 6 weeks before a 2.2; 95% CI, 1.5 to 3.2), and not significantly dif-
thrombotic event (odds ratio, 9.8; 95% CI, 7.0 to ferent in the periods of 13 to 18 weeks or 19 to
n engl j med 370;14nejm.orgapril 3, 2014 1311
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
6-week postpartum period, as compared with a
30 similar time period 1 year later, although abso-
29
28
lute risk increases were small after 6 weeks. As
27 compared with the absolute increase in risk dur-
26
25
ing the period within 6 weeks after delivery (22.1
24 cases per 100,000 deliveries), the absolute in-
23 crease during the postpartum period of 7 to 12
22
weeks was much smaller (3.0 cases per 100,000
Odds Ratio for Thrombotic Event
21
20 deliveries). During the latter period, odds ratios
19
18 for thrombosis were similar for women with rec-
17 ognized risk factors for thrombosis and those
16
15 without those risk factors, so the increased rela-
14 tive risk would be expected to be especially im-
13
12
portant among high-risk patients (e.g., those
11 with an inherited primary hypercoagulable state
10
9
or previous thrombosis).
8 To our knowledge, previous studies have not
7 reliably determined the relative risk of thrombo-
6
5 sis beyond 6 weeks after delivery. A population-
4 based analysis of pregnancy-related venous
3
2 thromboembolism over several decades included
1 events up to 3 months after delivery, but only
0 3 4 6 7 9 10 12 13 15 16 18 19 21 22 24 two cases were captured beyond 6 weeks, and
Weeks after Labor and Delivery relative risks for this period were not reported.5
In a population-based study of venous thrombo-
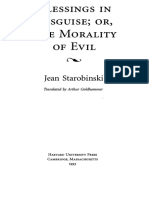
Figure 1. Risk of a Thrombotic Event, According to the Interval after Delivery. embolism after in vitro fertilization, thrombosis
Shown are the results of a post hoc exploratory analysis of the risk of a com rates between 7 weeks and 1 year after delivery
posite primary outcome of ischemic stroke, acute myocardial infarction, or were reported, but the study lacked suitable
venous thromboembolism across sequential 3-week periods after labor and nonpregnant control patients or intervals.26 In
delivery, as compared with each patients risk during the same period 1 year
another population-based study, there was no
later. The thrombotic risk was still increased during the period of 13 to 15 weeks
after delivery (odds ratio, 2.0; 95% CI, 1.1 to 3.6) but was no longer elevat significantly elevated risk of thrombosis between
ed in the period of 16 to 18 weeks after delivery (odds ratio, 1.0; 95% CI, 7 weeks and 1 year after delivery, but investiga-
0.6 to 1.8). The vertical lines indicate 95% confidence intervals. tors did not assess risks across discrete intervals
during that time.4 Two other studies suggested a
possibly heightened risk of venous thromboem-
24 weeks before a thrombotic event (Table 3). bolism between 7 and 12 weeks after delivery
This pattern was essentially unchanged in a nest- but lacked sufficient statistical power8 or had
ed analysis that included only patients who were imbalances between cases and controls, which
known to be alive and under observation for the probably resulted in an overestimation of post-
entire 1 year 24 weeks before the thrombotic partum risks.9
event. In a separate casecontrol analysis, women Despite this limited prior evidence, our find-
with a thrombotic event were more likely to have ing that increased risk for thrombosis persists
been hospitalized for labor and delivery within beyond 6 weeks after delivery has face validity.
the previous 7 to 12 weeks than to have been The magnitude of increased risk is high through-
hospitalized for another diagnosis (odds ratio, out the 6 weeks after delivery,2,5 and it is un-
1.9; 95% CI, 1.4 to 2.5) (data not shown). likely that this prothrombotic state would re-
solve suddenly. Our findings are consistent with
Discussion a more biologically plausible tapering of risk
through at least 12 weeks after delivery (Fig. 1).
Using administrative claims data from a large This pattern is concordant with data on labora-
state population, we found that the risk of a tory coagulation markers after delivery; most of
thrombotic event remained elevated beyond the these markers normalize by 6 weeks after deliv-
1312 n engl j med 370;14nejm.orgapril 3, 2014
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
Thrombotic Risk after 6-Week Postpartum Period
Table 3. Number and Rate of Deliveries during Sequential 6-Week Intervals Preceding a Thrombotic Event (Case-Crossover
Analysis).*
Time Interval after Labor Case Crossover Absolute Risk Difference Odds Ratio
and Delivery and Outcome Period Period (95% CI) (95% CI)
no. of events (rate per
100,000 deliveries)
Weeks 06
Stroke, myocardial infarction, or 354 (22.8) 36 (2.3) 20.4 (17.9 to 23.0) 9.8 (7.0 to 13.9)
venous thromboembolism
Stroke 96 (6.2) 13 (0.8) 5.3 (4.0 to 6.7) 7.4 (4.1 to 13.2)
Myocardial infarction 19 (1.2) 1 (0.1) 1.2 (0.5 to 1.8) 19.0 (2.5 to 141.9)
Venous thromboembolism 239 (15.4) 22 (1.4) 14.0 (11.9 to 16.1) 10.9 (7.0 to 16.8)
Stroke, myocardial infarction, venous 2013 (129.4) 92 (5.9) 123.5 (117.6 to 129.3) 21.9 (17.8 to 27.0)
thromboembolism, or other
Weeks 712
Stroke, myocardial infarction, or 76 (4.9) 35 (2.2) 2.6 (1.2 to 4.0) 2.2 (1.5 to 3.2)
venous thromboembolism
Stroke 12 (0.8) 8 (0.5) 0.3 (0.4 to 0.9) 1.5 (0.6 to 3.7)
Myocardial infarction 7 (0.5) 2 (0.1) 0.3 (0.1 to 0.8) 3.5 (0.7 to 16.8)
Venous thromboembolism 57 (3.7) 25 (1.6) 2.1 (0.9 to 3.3) 2.3 (1.4 to 3.6)
Stroke, myocardial infarction, venous 182 (11.7) 74 (4.8) 6.9 (4.9 to 9.0) 2.5 (1.9 to 3.2)
thromboembolism, or other
Weeks 1318
Stroke, myocardial infarction, or 48 (3.1) 36 (2.3) 0.8 (0.4 to 2.0) 1.3 (0.9 to 2.1)
venous thromboembolism
Stroke 11 (0.7) 9 (0.6) 0.1 (0.5 to 0.8) 1.2 (0.5 to 2.9)
Myocardial infarction 2 (0.1) 2 (0.1) 0 (0.3 to 0.3) 1.0 (0.1 to 7.1)
Venous thromboembolism 35 (2.3) 25 (1.6) 0.6 (0.4 to 1.7) 1.4 (0.8 to 2.3)
Stroke, myocardial infarction, venous 94 (6.0) 81 (5.2) 0.8 (0.9 to 2.6) 1.2 (0.9 to 1.6)
thromboembolism, or other
Weeks 1924
Stroke, myocardial infarction, or 46 (3.0) 53 (3.4) 0.4 (1.8 to 0.9) 0.9 (0.6 to 1.3)
venous thromboembolism
Stroke 15 (1.0) 15 (1.0) 0 (0.8 to 0.8) 1.0 (0.5 to 2.0)
Myocardial infarction 4 (0.3) 2 (0.1) 0.1 (0.2 to 0.5) 2.0 (0.4 to 10.9)
Venous thromboembolism 27 (1.7) 36 (2.3) 0.6 (1.6 to 0.5) 0.8 (0.5 to 1.2)
Stroke, myocardial infarction, venous 86 (5.5) 105 (6.7) 1.2 (3.0 to 0.6) 0.8 (0.6 to 1.1)
thromboembolism, or other
* Data for the case period are for the indicated interval before a first thrombotic event. Data for the crossover period are
for the indicated interval plus 1 year before a first thrombotic event.
ery, but some remain abnormal through at least supported by the consistency of our findings in a
8 to 12 weeks after delivery.27-29 confirmatory case-crossover analysis. Our study
The validity of our study is buttressed by its fully meets the assumptions of these crossover
crossover-cohort design, which allowed each designs, in that we modeled a transient, discrete
patient to serve as her own control and thus re- exposure with stable prevalence over time and
duced the unmeasured confounding that can an outcome that was defined by an acute event.30
occur with traditional casecontrol or cohort Limitations of our study require consideration,
studies.12 The validity of our study is further however. First, in the absence of prospective
n engl j med 370;14nejm.orgapril 3, 2014 1313
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
case ascertainment and detailed clinical informa- study period. Third, the sensitivities of the diag-
tion, some outcome events may have represented nosis codes that we used to determine risk fac-
delayed sequelae of previous thrombotic events. tors for thrombosis have not been validated, and
For example, an outpatient in whom venous therefore our subgroup analyses may not have
thromboembolism is diagnosed at 2 weeks after detected true interactions between specific risk
delivery who is then hospitalized with symptoms factors especially between the presence of a
of venous thromboembolism 8 weeks later would primary hypercoagulable state and smoking
have incorrectly appeared to have had a first and the duration of thrombotic risk after deliv-
thrombotic event at 10 weeks after delivery. This ery. Fourth, we lacked data from federal health
scenario would have artificially increased the ap- care facilities, which comprise 3.1% of the fa-
parent length of time between delivery and out- cilities in California.33
come, thereby upwardly biasing our estimates Current guidelines advise that high-risk pa-
for later postpartum periods. However, we think tients receive prophylactic anticoagulant therapy
that this possibility is unlikely to have substan- until 6 weeks after delivery, but these recommen-
tially affected our results. Although we may not dations are based largely on expert opinion.1
have captured some cases of venous thrombo- The duration of therapy that best balances the
embolism that were diagnosed entirely in the risk of thrombosis with the risk of bleeding34,35
outpatient setting, almost all diagnoses of ische remains uncertain.36 Our findings suggest that
mic stroke and acute myocardial infarction are the risks and benefits of continuing treatment
made in the emergency department and result in for high-risk women beyond 6 weeks after deliv-
hospitalization,31,32 and our analysis of these ery should be investigated. In addition, clinicians
arterial events alone was consistent with our over- who are evaluating possible symptoms of throm-
all analysis. Furthermore, our estimates of the bosis in postpartum women should recognize
magnitude of thrombotic risk within 6 weeks that risk remains increased for at least 12 weeks
after delivery closely overlap with those of previ- after delivery, although the absolute risk of throm-
ous studies that incorporated detailed clinical botic events beyond 6 weeks after delivery is low.
information,2,5 suggesting that we did not often The views expressed in this article are those of the authors and
do not necessarily represent the official views of the National
miss thrombotic events and incorrectly ascribe Institutes of Health (NIH).
them to later periods. Second, patients may have Supported by a grant from the National Institute of
been progressively lost to follow-up during the Neurological Disorders and Stroke of the NIH (K23NS082367, to
Dr. Kamel).
1 year 24 weeks after delivery owing to unre- Dr. Kamel reports receiving advisory board and lecture fees from
corded out-of-hospital deaths or emigration from Genentech; Dr. Devereux, receiving consulting fees from Merck;
California, and this would also have upwardly and Dr. Elkind, receiving consulting fees from Daiichi Sankyo,
Janssen, Biogen Idec, and Bristol-Myers Squibb/Pfizer, grant sup-
biased our estimates. However, we think that port from diaDexus and Bristol-Myers Squibb/Sanofi, and fees for
this is unlikely because we found the same re- providing expert testimony related to prescription treatments from
sults in a nested case-crossover analysis that was Merck/Organon, Novartis, and GlaxoSmithKline. No other poten-
tial conflict of interest relevant to this article was reported.
limited to patients who were known to be alive Disclosure forms provided by the authors are available with
and under observation throughout the entire the full text of this article at NEJM.org.
References
1. Bates SM, Greer IA, Middeldorp S, Bellocco R, Petersson G, Cnattingius S. KM, Nelson-Piercy C, Grainge MJ. Risk
Veenstra DL, Prabulos AM, Vandvik PO. Increased risks of circulatory diseases in of first venous thromboembolism in and
VTE, thrombophilia, antithrombotic ther late pregnancy and puerperium. Epidemi around pregnancy: a population-based
apy, and pregnancy: antithrombotic ther- ology 2001;12:456-60. cohort study. Br J Haematol 2012;156:366-
apy and prevention of thrombosis, 9th ed: 5. Heit JA, Kobbervig CE, James AH, 73.
American College of Chest Physicians evi- Petterson TM, Bailey KR, Melton LJ III. 9. Pomp ER, Lenselink AM, Rosendaal
dence-based clinical practice guidelines. Trends in the incidence of venous throm- FR, Doggen CJ. Pregnancy, the postpar-
Chest 2012;141:Suppl:691S-736S. boembolism during pregnancy or post- tum period and prothrombotic defects:
2. Kittner SJ, Stern BJ, Feeser BR, et al. partum: a 30-year population-based study. risk of venous thrombosis in the MEGA
Pregnancy and the risk of stroke. N Engl J Ann Intern Med 2005;143:697-706. study. J Thromb Haemost 2008;6:632-7.
Med 1996;335:768-74. 6. Jaigobin C, Silver FL. Stroke and preg- 10. Nazziola E, Elkind MS. Dural sinus
3. James AH, Jamison MG, Biswas MS, nancy. Stroke 2000;31:2948-51. thrombosis presenting three months post-
Brancazio LR, Swamy GK, Myers ER. 7. James AH, Bushnell CD, Jamison MG, partum. Ann Emerg Med 2003;42:592-5.
Acute myocardial infarction in pregnancy: Myers ER. Incidence and risk factors for 11. Maclure M, Mittleman MA. Should we
a United States population-based study. stroke in pregnancy and the puerperium. use a case-crossover design? Annu Rev
Circulation 2006;113:1564-71. Obstet Gynecol 2005;106:509-16. Public Health 2000;21:193-221.
4. Salonen Ros H, Lichtenstein P, 8. Sultan AA, West J, Tata LJ, Fleming 12. Suissa S. The case-time-control de-
1314 n engl j med 370;14nejm.orgapril 3, 2014
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
Thrombotic Risk after 6-Week Postpartum Period
sign: further assumptions and conditions. 2012;141:Suppl:7S-47S. [Errata, Chest 2012; lysis in the normal puerperium. Gynecol
Epidemiology 1998;9:441-5. 141:1129, 2012;142:1698.] Obstet Invest 1985;20:37-44.
13. U.S. Census Bureau. California state 22. Scott CA, Bewley S, Rudd A, et al. 30. Delaney JA, Suissa S. The case-cross-
and county QuickFacts (http://quickfacts Incidence, risk factors, management, and over study design in pharmacoepidemiol-
.census.gov/qfd/states/06000.html). outcomes of stroke in pregnancy. Obstet ogy. Stat Methods Med Res 2009;18:53-65.
14. Agency for Healthcare Research and Gynecol 2012;120:318-24. 31. Jauch EC, Saver JL, Adams HP Jr, et al.
Quality. Healthcare Cost and Utilization 23. James AH, Jamison MG, Brancazio Guidelines for the early management of
Project home page (http://hcupnet.ahrq LR, Myers ER. Venous thromboembolism patients with acute ischemic stroke:
.gov). during pregnancy and the postpartum a guideline for healthcare professionals
15. California Office of Statewide Health period: incidence, risk factors, and mor- from the American Heart Association/
Planning and Development home page tality. Am J Obstet Gynecol 2006;194: American Stroke Association. Stroke 2013;
(http://www.oshpd.ca.gov/). 1311-5. 44:870-947.
16. Bushnell CD, Jamison M, James AH. 24. Fang MC, Go AS, Chang Y, et al. A new 32. Anderson JL, Adams CD, Antman EM,
Migraines during pregnancy linked to risk scheme to predict warfarin-associat- et al. 2012 ACCF/AHA focused update in-
stroke and vascular diseases: US popula- ed hemorrhage: the ATRIA (Anticoagu corporated into the ACCF/AHA 2007
tion based case-control study. BMJ 2009; lation and Risk Factors in Atrial Fibrilla guidelines for the management of pa-
338:b664. tion) Study. J Am Coll Cardiol 2011;58: tients with unstable angina/non-ST-eleva-
17. California Department of Public 395-401. tion myocardial infarction: a report of the
Health. Birth statistical data tables (http:// 25. Elixhauser A, Steiner C, Harris DR, American College of Cardiology Founda
www.cdph.ca.gov/data/statistics/Pages/ Coffey RM. Comorbidity measures for use tion/American Heart Association Task
StatewideBirthStatisticalDataTables.aspx). with administrative data. Med Care 1998; Force on Practice Guidelines. Circulation
18. Tirschwell DL, Longstreth WT Jr. 36:8-27. 2013;127(23):e663-e828.
Validating administrative data in stroke 26. Henriksson P, Westerlund E, Walln 33. American Hospital Association.
research. Stroke 2002;33:2465-70. H, Brandt L, Hovatta O, Ekbom A. Inci Annual survey: fast facts on US hospitals
19. Kiyota Y, Schneeweiss S, Glynn RJ, dence of pulmonary and venous thrombo- (http://www.aha.org/research/rc/stat
Cannuscio CC, Avorn J, Solomon DH. embolism in pregnancies after in vitro -studies/fast-facts.shtml).
Accuracy of Medicare claims-based diag- fertilisation: cross sectional study. BMJ 34. Eikelboom JW, Quinlan DJ, Douketis
nosis of acute myocardial infarction: esti- 2013;346:e8632. JD. Extended-duration prophylaxis against
mating positive predictive value on the 27. Louden KA, Broughton Pipkin F, Hep venous thromboembolism after total hip
basis of review of hospital records. Am tinstall S, Fox SC, Mitchell JR, Symonds or knee replacement: a meta-analysis of
Heart J 2004;148:99-104. EM. A longitudinal study of platelet be- the randomised trials. Lancet 2001;358:
20. White RH, Gettner S, Newman JM, haviour and thromboxane production in 9-15.
Trauner KB, Romano PS. Predictors of re- whole blood in normal pregnancy and the 35. Hull RD, Schellong SM, Tapson VF,
hospitalization for symptomatic venous puerperium. Br J Obstet Gynaecol 1990;97: et al. Extended-duration venous thrombo-
thromboembolism after total hip arthro- 1108-14. embolism prophylaxis in acutely ill medi-
plasty. N Engl J Med 2000;343:1758-64. 28. Kjellberg U, Andersson NE, Rosn S, cal patients with recently reduced mobil-
21. Guyatt GH, Akl EA, Crowther M, Tengborn L, Hellgren M. APC resistance ity: a randomized trial. Ann Intern Med
Gutterman DD, Schuunemann HJ. Execu and other haemostatic variables during 2010;153:8-18.
tive summary: antithrombotic therapy and pregnancy and puerperium. Thromb 36. Middeldorp S. Thrombosis in women:
prevention of thrombosis, 9th ed: Amer Haemost 1999;81:527-31. what are the knowledge gaps in 2013?
ican College of Chest Physicians evidence- 29. Dahlman T, Hellgren M, Blombck M. J Thromb Haemost 2013;11:Suppl 1:180-91.
based clinical practice guidelines. Chest Changes in blood coagulation and fibrino- Copyright 2014 Massachusetts Medical Society.
receive immediate notification when an article
is published online first
To be notified by e-mail when Journal articles
are published Online First, sign up at NEJM.org.
n engl j med 370;14nejm.orgapril 3, 2014 1315
The New England Journal of Medicine
Downloaded from nejm.org on April 26, 2015. For personal use only. No other uses without permission.
Copyright 2014 Massachusetts Medical Society. All rights reserved.
También podría gustarte
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Elements of Short Story WORKBOOKDocumento26 páginasElements of Short Story WORKBOOKDavid Velez Gonzalez100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- LNAT EssayDocumento2 páginasLNAT EssayFaisal . BathawabAún no hay calificaciones
- Quadratic EquationsDocumento40 páginasQuadratic EquationsWeb Books100% (6)
- Flat Glass-Pilkington-2009finalDocumento74 páginasFlat Glass-Pilkington-2009finalKancharla AnandAún no hay calificaciones
- Blessings in DisguiseDocumento238 páginasBlessings in DisguiseAJ HassanAún no hay calificaciones
- Chapter 1 A CULINARY HISTORYDocumento10 páginasChapter 1 A CULINARY HISTORYMrinalini KrishnanAún no hay calificaciones
- Why There Has Been No Brandies Brief in India? Challenges To Socio-Legal Research in IndiaDocumento2 páginasWhy There Has Been No Brandies Brief in India? Challenges To Socio-Legal Research in IndiaSubhaprad MohantyAún no hay calificaciones
- Deloitte IT Governance SurveyDocumento20 páginasDeloitte IT Governance Surveymrehan2k2Aún no hay calificaciones
- List of Astrology BooksDocumento19 páginasList of Astrology BooksChetan SharmaAún no hay calificaciones
- Alfred Nobel and The Nobel PrizesDocumento17 páginasAlfred Nobel and The Nobel PrizesElizabethDarcyAún no hay calificaciones
- Waste Segregator ReportDocumento33 páginasWaste Segregator ReportVinodNKumar25% (4)
- Dario Great Wall of China Lesson PlanDocumento3 páginasDario Great Wall of China Lesson Planapi-297914033Aún no hay calificaciones
- Mabini Colleges, Inc: College of Education Daet, Camarines NorteDocumento8 páginasMabini Colleges, Inc: College of Education Daet, Camarines NorteFrancia BalaneAún no hay calificaciones
- High School Kids Science Fiction Short StoriesDocumento5 páginasHigh School Kids Science Fiction Short StoriesHarshal bhardwaj100% (1)
- Central Limit TheoremDocumento46 páginasCentral Limit TheoremAneesh Gopinath 2027914Aún no hay calificaciones
- ENFSIDocumento8 páginasENFSIkmrdAún no hay calificaciones
- Evermotion Archmodels Vol 40 PDFDocumento2 páginasEvermotion Archmodels Vol 40 PDFJustinAún no hay calificaciones
- CDP MCQs - Child Development & Pedagogy (CDP) MCQ Questions With AnswerDocumento4 páginasCDP MCQs - Child Development & Pedagogy (CDP) MCQ Questions With AnswerPallav JainAún no hay calificaciones
- Goodrich 6e Ch03 Arrays PDFDocumento12 páginasGoodrich 6e Ch03 Arrays PDFArjun SinghAún no hay calificaciones
- The Essential Guide To Developing A Social Recruiting StrategyDocumento48 páginasThe Essential Guide To Developing A Social Recruiting Strategysubzzz222Aún no hay calificaciones
- Extra Counting ProblemsDocumento25 páginasExtra Counting ProblemsWilson ZhangAún no hay calificaciones
- Class IfDocumento9 páginasClass IfDavidRavenMoonAún no hay calificaciones
- Ethical Issues in SupervisionDocumento10 páginasEthical Issues in SupervisionBiona FranciscoAún no hay calificaciones
- Globalisation, Cosmopolitanism and EcologicalDocumento16 páginasGlobalisation, Cosmopolitanism and EcologicalRidhimaSoniAún no hay calificaciones
- Conditional Power of One Proportion Tests PDFDocumento7 páginasConditional Power of One Proportion Tests PDFscjofyWFawlroa2r06YFVabfbajAún no hay calificaciones
- Traffic Analysis For Project San AntonioDocumento3 páginasTraffic Analysis For Project San AntonioLoraine AnnAún no hay calificaciones
- 18 SSBDocumento162 páginas18 SSBapi-3806887Aún no hay calificaciones
- Teoria Do MSR ADocumento4 páginasTeoria Do MSR AAlexandre Valeriano da SilvaAún no hay calificaciones
- Primate City & Rank Size Rule: O P A DDocumento7 páginasPrimate City & Rank Size Rule: O P A DOmkar G. ParishwadAún no hay calificaciones
- Harrah's Entertainment Inc: Submitted To: Prof. Shubhamoy DeyDocumento6 páginasHarrah's Entertainment Inc: Submitted To: Prof. Shubhamoy DeyAbhinav UtkarshAún no hay calificaciones