También podría gustarte
- Selection of Teeth & Arrangement of Teeth: Praveen V BadwaikDocumento46 páginasSelection of Teeth & Arrangement of Teeth: Praveen V BadwaikPraveen BadwaikAún no hay calificaciones
- Effective Communications HandoutDocumento1 páginaEffective Communications HandoutSalai Thangte LaizoZanniatAún no hay calificaciones
- L3 Abutments in FPD 13-1-22Documento19 páginasL3 Abutments in FPD 13-1-22Ju JuAún no hay calificaciones
- Annex F - Assessment of Oral Mucosal TissueDocumento2 páginasAnnex F - Assessment of Oral Mucosal TissueGowriAún no hay calificaciones
- Oral Biology 1 Lab Manual: Faculty of DentistryDocumento41 páginasOral Biology 1 Lab Manual: Faculty of DentistryMustafa SaßerAún no hay calificaciones
- Lecture 5 Equine DentistryDocumento38 páginasLecture 5 Equine Dentistryannelle0219Aún no hay calificaciones
- Ponticos OvoidesDocumento9 páginasPonticos OvoidesJuan Jose Stuven RodriguezAún no hay calificaciones
- Make A List of 50 Words Used in The World of DentistryDocumento1 páginaMake A List of 50 Words Used in The World of DentistryGrecia BecerraAún no hay calificaciones
- Myofunctional Orthodontic Evaluation FormDocumento1 páginaMyofunctional Orthodontic Evaluation FormSurya DinataAún no hay calificaciones
- The Wax Try-InDocumento45 páginasThe Wax Try-Inmohammedhs905Aún no hay calificaciones
- Swallowing ChecklistsDocumento5 páginasSwallowing ChecklistsTaylor MayAún no hay calificaciones
- Non Carious LesionsDocumento70 páginasNon Carious LesionsSayak GuptaAún no hay calificaciones
- Chronology & MorphologyDocumento30 páginasChronology & MorphologyAhsan Ul Kayum BhuiyanAún no hay calificaciones
- Single Complete DentureDocumento20 páginasSingle Complete DentureslidezbuzzAún no hay calificaciones
- Sample NOT FOR Reproduction: Interproximal ReductionDocumento2 páginasSample NOT FOR Reproduction: Interproximal ReductionhemaadriAún no hay calificaciones
- CAS and Hearing Loss Handout FurnariDocumento27 páginasCAS and Hearing Loss Handout FurnariRoelen F (Miss F)Aún no hay calificaciones
- Health Card FrontDocumento3 páginasHealth Card FrontCarlaGomezAún no hay calificaciones
- RPD DesignDocumento15 páginasRPD DesignRizky FebiyantiAún no hay calificaciones
- In Consortium With N. Bacalso Ave. Cor Panganiban ST., 6000 Cebu City, Cebu, Philippines Tel. Nos. (032) 316-5128/ (032) 4186105 Email AddressDocumento5 páginasIn Consortium With N. Bacalso Ave. Cor Panganiban ST., 6000 Cebu City, Cebu, Philippines Tel. Nos. (032) 316-5128/ (032) 4186105 Email AddressCarl Jayson LeysonAún no hay calificaciones
- ResumeDocumento1 páginaResumeapi-398428706Aún no hay calificaciones
- Prosthodontics: Dental Assistant Diploma ProgramDocumento33 páginasProsthodontics: Dental Assistant Diploma ProgrambeyAún no hay calificaciones
- Othodontic Case ReportDocumento3 páginasOthodontic Case Reportالعمري العمريAún no hay calificaciones
- English For DentistsDocumento5 páginasEnglish For DentistsPalmira Aragonés RubioAún no hay calificaciones
- Tooth Surfaces & ThirdsDocumento54 páginasTooth Surfaces & ThirdsdrnaglaaAún no hay calificaciones
- Learn More Today!: Tongue-Tie Symposium 2019Documento1 páginaLearn More Today!: Tongue-Tie Symposium 2019Anonymous GtVzVadPAún no hay calificaciones
- Medidas IvoclarDocumento5 páginasMedidas IvoclarKarina OjedaAún no hay calificaciones
- Phonetics in Complete Denture-3670Documento5 páginasPhonetics in Complete Denture-3670Najeeb UllahAún no hay calificaciones
- Post-Insertio N Denture Problem S: Complaints On ComfortDocumento3 páginasPost-Insertio N Denture Problem S: Complaints On ComfortbiancaAún no hay calificaciones
- ATE Brandt 062306 CDocumento81 páginasATE Brandt 062306 CYasser El-AliAún no hay calificaciones
- Try in Appointment Post Insertion Instructions ProsthoDocumento24 páginasTry in Appointment Post Insertion Instructions ProsthoFourthMolar.comAún no hay calificaciones
- Dental MorfologiDocumento43 páginasDental MorfologiAvirna IdayantiAún no hay calificaciones
- Junior Prosthodontics III AIDM SGDocumento16 páginasJunior Prosthodontics III AIDM SGbenrejebyahiaAún no hay calificaciones
- Variants of Talon Cusp (Dens2017Documento2 páginasVariants of Talon Cusp (Dens2017Hukjvccx JjyfdxxvbAún no hay calificaciones
- The Try-In Appointment: Dr. Salwan Al-HamdaniDocumento17 páginasThe Try-In Appointment: Dr. Salwan Al-Hamdanimohammedhs905Aún no hay calificaciones
- Prosthodontics2 2Documento5 páginasProsthodontics2 2Hannah RosalesAún no hay calificaciones
- Lecture 3 - English ConsonantsDocumento5 páginasLecture 3 - English ConsonantsAtul JaniAún no hay calificaciones
- Biologic Esthetics by Gingival Framework Desing Part 2 Gingival EstheticsDocumento13 páginasBiologic Esthetics by Gingival Framework Desing Part 2 Gingival EstheticsAna Veronica100% (2)
- Topical and Structurated Syllabus Corrected.1Documento10 páginasTopical and Structurated Syllabus Corrected.1Kikis Dom100% (1)
- مريم بروستDocumento29 páginasمريم بروستOmar QasimAún no hay calificaciones
- Dental Risk Assessment FormDocumento2 páginasDental Risk Assessment FormCharlie SumagaysayAún no hay calificaciones
- Which Prosthesis Converted.Documento17 páginasWhich Prosthesis Converted.Khan MustafaAún no hay calificaciones
- Prescott Cosmetic Dentist Prescott Cosmetic DentistDocumento54 páginasPrescott Cosmetic Dentist Prescott Cosmetic DentistDavid HerbertAún no hay calificaciones
- Articulation and Phonological Processess SummarisedDocumento2 páginasArticulation and Phonological Processess SummarisedSuné GreeffAún no hay calificaciones
- ZirconiaDocumento674 páginasZirconiaKalpanaAún no hay calificaciones
- Oral HProfile T&NTPDocumento1 páginaOral HProfile T&NTPMaria Fatima ArnaizAún no hay calificaciones
- Detecting Oral Cancer: A Guide For Health Care ProfessionalsDocumento19 páginasDetecting Oral Cancer: A Guide For Health Care ProfessionalsShabeel PnAún no hay calificaciones
- 17 Keywords To Learn For Going To The Dentist in ChinaDocumento2 páginas17 Keywords To Learn For Going To The Dentist in ChinaMichael Yang TangAún no hay calificaciones
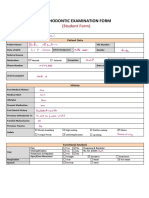
- Ortho Examinathion Form Students Copy Cast AnalysisDocumento5 páginasOrtho Examinathion Form Students Copy Cast AnalysisAseel RoziAún no hay calificaciones
- Complete Dentures - Trial Denture AppointmentDocumento20 páginasComplete Dentures - Trial Denture Appointmentjohn mwambuAún no hay calificaciones
- Dental FlossDocumento1 páginaDental FlossAshnaAún no hay calificaciones
- 10-Post Insertion Problems and ComplaintsDocumento188 páginas10-Post Insertion Problems and ComplaintsZachary DuongAún no hay calificaciones
- Speech Organs PDFDocumento25 páginasSpeech Organs PDFVivian0% (2)
- Permanent Dental Record: Name of Hospital: AddressDocumento1 páginaPermanent Dental Record: Name of Hospital: AddresseroshAún no hay calificaciones
- Dental 20 Vocabulary 20 FinalDocumento2 páginasDental 20 Vocabulary 20 FinalAmira IdrisAún no hay calificaciones
- B - Cracked Tooth SyndromeDocumento8 páginasB - Cracked Tooth SyndromeDavid TaylorAún no hay calificaciones
- Fixed Partial Denture/: Gigi Tiruan JembatanDocumento25 páginasFixed Partial Denture/: Gigi Tiruan JembatanKyrkAún no hay calificaciones
- Dental Charting V0.5 July 2020Documento12 páginasDental Charting V0.5 July 2020marizanunez0211Aún no hay calificaciones
- Periapical Assessment Report: Bright Teeth ClinicDocumento2 páginasPeriapical Assessment Report: Bright Teeth ClinicGaurav SrivastavaAún no hay calificaciones
- 20 Minute Phonemic Training for Dyslexia, Auditory Processing, and Spelling: A Complete Resource for Speech Pathologists, Intervention Specialists, and Reading TutorsDe Everand20 Minute Phonemic Training for Dyslexia, Auditory Processing, and Spelling: A Complete Resource for Speech Pathologists, Intervention Specialists, and Reading TutorsAún no hay calificaciones
- Oral Health Assessment and Review: Guidance Implementation SummaryDocumento4 páginasOral Health Assessment and Review: Guidance Implementation SummarymebibegAún no hay calificaciones
- Bisphosphonates Patient Leaflet - Accessible VersionDocumento2 páginasBisphosphonates Patient Leaflet - Accessible VersionmebibegAún no hay calificaciones
- The UK National Cohort Study Evaluating Dental Vocational TrainingDocumento4 páginasThe UK National Cohort Study Evaluating Dental Vocational TrainingmebibegAún no hay calificaciones
- Patient History Update: CHI NumberDocumento1 páginaPatient History Update: CHI NumbermebibegAún no hay calificaciones
- Prevention and Management of Caries in General Dental PracticeDocumento2 páginasPrevention and Management of Caries in General Dental PracticemebibegAún no hay calificaciones
- Prevention of Gum Disease: Diabetes and Your Oral HealthDocumento3 páginasPrevention of Gum Disease: Diabetes and Your Oral HealthmebibegAún no hay calificaciones
- MR Steve Turner, DR Steve Macgillivray, Ms Sheela TripatheeDocumento1 páginaMR Steve Turner, DR Steve Macgillivray, Ms Sheela TripatheemebibegAún no hay calificaciones
- Radiographic Form 9 PDFDocumento1 páginaRadiographic Form 9 PDFmebibegAún no hay calificaciones
- Assessment of Head and Neck Form 5: II I IIDocumento1 páginaAssessment of Head and Neck Form 5: II I IImebibegAún no hay calificaciones
- Prevention of Gum Disease: Your Oral HealthDocumento3 páginasPrevention of Gum Disease: Your Oral HealthmebibegAún no hay calificaciones
- Social and Dental History Form 2: CHI NumberDocumento2 páginasSocial and Dental History Form 2: CHI NumbermebibegAún no hay calificaciones
- Patient's Personal Details Form 1: CHI NumberDocumento2 páginasPatient's Personal Details Form 1: CHI NumbermebibegAún no hay calificaciones
- Oral Health Assessment and Review Checklist: CHI NumberDocumento1 páginaOral Health Assessment and Review Checklist: CHI NumbermebibegAún no hay calificaciones
- Patient Review and Personal Care Plan: Dentist's Details SurnameDocumento2 páginasPatient Review and Personal Care Plan: Dentist's Details SurnamemebibegAún no hay calificaciones
- Local Contacts For Advice and Referral: Provider Contact DetailsDocumento2 páginasLocal Contacts For Advice and Referral: Provider Contact DetailsmebibegAún no hay calificaciones
- Aggressive Periodontitis: Localized & Generalized Forms by SamDocumento24 páginasAggressive Periodontitis: Localized & Generalized Forms by SammebibegAún no hay calificaciones
- VgsbwgyhcxbDocumento24 páginasVgsbwgyhcxbmebibegAún no hay calificaciones
- Tarrson Family Endowed Chair in PeriodonticsDocumento34 páginasTarrson Family Endowed Chair in Periodonticsapi-3827876Aún no hay calificaciones
- GFHHDocumento11 páginasGFHHmebibegAún no hay calificaciones
- FvtgbyhnujDocumento21 páginasFvtgbyhnujmebibegAún no hay calificaciones
- Downs Analysis: SL Parameters Down's Mean Observed Values InferencesDocumento9 páginasDowns Analysis: SL Parameters Down's Mean Observed Values Inferencesmebibeg50% (4)
- Contents:-: Acrylic Resin Silicones Tissue Conditioners Conclusion ReferencesDocumento6 páginasContents:-: Acrylic Resin Silicones Tissue Conditioners Conclusion ReferencesmebibegAún no hay calificaciones
- Siemens, British Gas Invest in Broadband-Over-Powerline Company For Smart GridDocumento3 páginasSiemens, British Gas Invest in Broadband-Over-Powerline Company For Smart GridmebibegAún no hay calificaciones
- Historical BackgroundDocumento5 páginasHistorical BackgroundmebibegAún no hay calificaciones
- IPS Emax Press Ingot RangeDocumento6 páginasIPS Emax Press Ingot Rangewuhan lalala100% (1)
- The Viazis Classification of Malocclusion: Journal of Dental Health Oral Disorders & TherapyDocumento9 páginasThe Viazis Classification of Malocclusion: Journal of Dental Health Oral Disorders & TherapyWilmer Yanquen VillarrealAún no hay calificaciones
- Water LaceDocumento67 páginasWater LaceRekha BipinAún no hay calificaciones
- Making An AppointmentDocumento20 páginasMaking An AppointmentRefta Sekar DeviAún no hay calificaciones
- Dental Caries: Signs and SymptomsDocumento13 páginasDental Caries: Signs and SymptomsGeorgiana IlincaAún no hay calificaciones
- AlencarCMetal 2021Documento12 páginasAlencarCMetal 2021Nabila RizkikaAún no hay calificaciones
- Dent05 p0393Documento7 páginasDent05 p0393Liga Odontopediatria RondonienseAún no hay calificaciones
- Epidemiology of Dental Caries When Structure and Context MatterDocumento7 páginasEpidemiology of Dental Caries When Structure and Context MatterHUGO GOUVEIAAún no hay calificaciones
- Multidisciplinary Approach For The Closure of Multiple Diastemata With Composite ResinDocumento15 páginasMultidisciplinary Approach For The Closure of Multiple Diastemata With Composite ResinCentro Dental IntegralAún no hay calificaciones
- Complete Denture - The BPS Way: January 2014Documento8 páginasComplete Denture - The BPS Way: January 2014PhanQuangHuyAún no hay calificaciones
- CD CareDocumento8 páginasCD CareAkshayAún no hay calificaciones
- An Evidence-Based Reference: Diseases and Conditions in DentistryDocumento1 páginaAn Evidence-Based Reference: Diseases and Conditions in DentistryGabriel LazarAún no hay calificaciones
- Articol ImplantologieDocumento6 páginasArticol ImplantologieAna MoraruAún no hay calificaciones
- PRD 14 5 Scipioni 6 PDFDocumento10 páginasPRD 14 5 Scipioni 6 PDFAlla MushkeyAún no hay calificaciones
- Poor Oral Health Including Active Caries in 187 UK Professional Male Football Players: Clinical Dental Examination Performed by DentistsDocumento6 páginasPoor Oral Health Including Active Caries in 187 UK Professional Male Football Players: Clinical Dental Examination Performed by DentistsJohnny CHAún no hay calificaciones
- Contemporary Partial Denture DesignsDocumento9 páginasContemporary Partial Denture DesignsmujtabaAún no hay calificaciones
- Oral Health Among Junior High School Student in Saints John and Paul Educational FoundationDocumento15 páginasOral Health Among Junior High School Student in Saints John and Paul Educational FoundationDat boiAún no hay calificaciones
- Reliability and Validity of T-Scan and 3D Intraoral Scanning For Measuring The Occlusal Contact AreaDocumento7 páginasReliability and Validity of T-Scan and 3D Intraoral Scanning For Measuring The Occlusal Contact AreaananthAún no hay calificaciones
- Trends in ProsthodonticsDocumento14 páginasTrends in ProsthodonticsAeman ElkezzaAún no hay calificaciones
- 1-Pin Retained RestorationDocumento79 páginas1-Pin Retained Restorationemad helalAún no hay calificaciones
- Wiley EssentialsofDentalPhotography 978-1-119 31214 7Documento2 páginasWiley EssentialsofDentalPhotography 978-1-119 31214 7Lilla NovakAún no hay calificaciones
- KararyDocumento39 páginasKararyوليد خالدAún no hay calificaciones
- Section 032 RPD ImpressionsDocumento3 páginasSection 032 RPD Impressionsapi-3710948Aún no hay calificaciones
- Organisational Change, Environmental and Ethical IssuesDocumento20 páginasOrganisational Change, Environmental and Ethical IssuesCvetozar MilanovAún no hay calificaciones
- Dental Caries A Microbiological ApproachDocumento15 páginasDental Caries A Microbiological ApproachAnnabella NatashaAún no hay calificaciones
- Antimicrobial Effectiveness of Cetylpyridinium Chloride and Zinc Chloride-Containing Mouthrinses On Bacteria of Halitosis and Peri-Implant DiseaseDocumento7 páginasAntimicrobial Effectiveness of Cetylpyridinium Chloride and Zinc Chloride-Containing Mouthrinses On Bacteria of Halitosis and Peri-Implant DiseasePhuong ThaoAún no hay calificaciones
- Dentaltown 2018marchDocumento113 páginasDentaltown 2018marchDanutz BalanAún no hay calificaciones
- Occlusion MCQDocumento41 páginasOcclusion MCQAmar Bhochhibhoya72% (29)
- Class 1 +class1 With Extention & Class V (Amalgam)Documento22 páginasClass 1 +class1 With Extention & Class V (Amalgam)Vinay PandeyAún no hay calificaciones
- Influence of Occlusal Rest Position and Clasp Design On Movement of Abutment Teeth - Journal of Prosthetic Dentistry PDFDocumento2 páginasInfluence of Occlusal Rest Position and Clasp Design On Movement of Abutment Teeth - Journal of Prosthetic Dentistry PDFdrgayen6042Aún no hay calificaciones