También podría gustarte
- Oet GuideDocumento109 páginasOet GuideBünyamin Emer100% (1)
- RCDSO Guidelines Role of OpioidsDocumento16 páginasRCDSO Guidelines Role of OpioidsMonaAún no hay calificaciones
- Iggy Med Surg Test Bank Chapter 005Documento19 páginasIggy Med Surg Test Bank Chapter 005Tracy Bartell80% (10)
- Synopsis: ST John'S College of NursingDocumento19 páginasSynopsis: ST John'S College of NursingsyarifaAún no hay calificaciones
- Effectivemanagementof Painandanxietyforthe Pediatricpatientintheemergency DepartmentDocumento12 páginasEffectivemanagementof Painandanxietyforthe Pediatricpatientintheemergency DepartmentGisele Elise MeninAún no hay calificaciones
- Manejo Del Dolor en RNDocumento30 páginasManejo Del Dolor en RNtadessetogaAún no hay calificaciones
- Neonatal Pain Management DissertationDocumento8 páginasNeonatal Pain Management DissertationWillSomeoneWriteMyPaperForMeNorman100% (1)
- Pediatricpainmanagement: Aarti Gaglani,, Toni GrossDocumento12 páginasPediatricpainmanagement: Aarti Gaglani,, Toni GrossCarlos Manuel EscolasticoAún no hay calificaciones
- Review Article: Pain in Children: Assessment and Nonpharmacological ManagementDocumento12 páginasReview Article: Pain in Children: Assessment and Nonpharmacological Management1150019052 KHASAN HAQQUL AMINAún no hay calificaciones
- Pain Neuroscience Education StateDocumento17 páginasPain Neuroscience Education StateToni DAún no hay calificaciones
- Harrison Prevention and Management of Pain and Stress in The Neonate 2015Documento8 páginasHarrison Prevention and Management of Pain and Stress in The Neonate 2015Sasha Hidayat FullAún no hay calificaciones
- Current Practice and Recent Advances in Pediatric Pain ManagementDocumento15 páginasCurrent Practice and Recent Advances in Pediatric Pain ManagementSyane TitaleyAún no hay calificaciones
- Cara PresentasiDocumento9 páginasCara PresentasiRamadhan SaAún no hay calificaciones
- Original Research Using Guided Imagery To Manage.25Documento11 páginasOriginal Research Using Guided Imagery To Manage.25wilmaAún no hay calificaciones
- Assessment of Neonatal Pain UPTODATE 2015Documento15 páginasAssessment of Neonatal Pain UPTODATE 2015Redina Tuya RamirezAún no hay calificaciones
- 1 s2.0 S1071909116300225 MainDocumento12 páginas1 s2.0 S1071909116300225 MainzumeeeAún no hay calificaciones
- Acute Pain Management in ChildrenDocumento20 páginasAcute Pain Management in Childrenfuka priesleyAún no hay calificaciones
- Effect of Active and Passive Distraction On Decreasing Pain Associated With Painful Medical Procedures Among School Aged ChildrenDocumento11 páginasEffect of Active and Passive Distraction On Decreasing Pain Associated With Painful Medical Procedures Among School Aged ChildrenTadea YasintaAún no hay calificaciones
- Effecttive Analgesia PD Imunisasi AnakDocumento10 páginasEffecttive Analgesia PD Imunisasi Anakmechi_ghisyaAún no hay calificaciones
- Bahan Tesin Pain in ChildrenDocumento11 páginasBahan Tesin Pain in ChildrenWiwit ClimberAún no hay calificaciones
- Acute Pediatric PainDocumento7 páginasAcute Pediatric PainsolidchessAún no hay calificaciones
- P AcutepainmgmtDocumento5 páginasP AcutepainmgmtLeticia Quiñonez VivasAún no hay calificaciones
- Pain Management in Infants - Children - AdolescentsDocumento9 páginasPain Management in Infants - Children - AdolescentsOxana Turcu100% (1)
- Pediatric Nursing Surgical NursingDocumento19 páginasPediatric Nursing Surgical NursingMelany KojachiAún no hay calificaciones
- Prevention and Management of Procedural Pain in The Neonate An U 2016Documento13 páginasPrevention and Management of Procedural Pain in The Neonate An U 2016Indra WijayaAún no hay calificaciones
- Pain Management Concept Analysis1Documento10 páginasPain Management Concept Analysis1darylablackman100% (1)
- Atraumatic Care: A Device To Reduce Pain in The Pediatric Population During Painful Ambulatory ProceduresDocumento4 páginasAtraumatic Care: A Device To Reduce Pain in The Pediatric Population During Painful Ambulatory Proceduresfikmanajemen 2018Aún no hay calificaciones
- .Dolor Neonato TradDocumento10 páginas.Dolor Neonato TradAsdrubal MontañoAún no hay calificaciones
- The Influence of An Accredited Pediatric Emergency Medicine Program On The Management of Pediatric Pain and AnxietyDocumento5 páginasThe Influence of An Accredited Pediatric Emergency Medicine Program On The Management of Pediatric Pain and AnxietyLotta AyuniyahAún no hay calificaciones
- Knowledge and Attitudes of Pediatric Clinicians Regarding Pediatric Pain ManagementDocumento11 páginasKnowledge and Attitudes of Pediatric Clinicians Regarding Pediatric Pain ManagementIkek StanzaAún no hay calificaciones
- Post Operative Pain Management in Paediatric Patients: Dr. R. P. GehdooDocumento9 páginasPost Operative Pain Management in Paediatric Patients: Dr. R. P. GehdooT RonaskyAún no hay calificaciones
- Jurnal AnakDocumento7 páginasJurnal AnakAbdu RahmanAún no hay calificaciones
- The Fifth Vital Sign Implementation PDFDocumento8 páginasThe Fifth Vital Sign Implementation PDFTeten RustendiAún no hay calificaciones
- JournalDocumento1 páginaJournalCheska YsabelleAún no hay calificaciones
- Nursing Thesis On Pain ManagementDocumento8 páginasNursing Thesis On Pain Managementashleythomaslafayette100% (2)
- 17 Shaw - Pediatric Pall Pain and Symptom MXDocumento6 páginas17 Shaw - Pediatric Pall Pain and Symptom MXRina WahyuniAún no hay calificaciones
- E607 FullDocumento10 páginasE607 FullCalvin AffendyAún no hay calificaciones
- Effects of Distraction On Children's Pain and Distress During Medical Procedures A Meta-AnalysisDocumento4 páginasEffects of Distraction On Children's Pain and Distress During Medical Procedures A Meta-AnalysisMiguel TuriniAún no hay calificaciones
- La Literature ReviewDocumento8 páginasLa Literature Reviewapi-640993798Aún no hay calificaciones
- Chronic Pain Thesis PDFDocumento5 páginasChronic Pain Thesis PDFtehuhevet1l2100% (2)
- Synthesis PaperDocumento10 páginasSynthesis Paperapi-485472556Aún no hay calificaciones
- Thesis On Pain ManagementDocumento5 páginasThesis On Pain ManagementWhatShouldIWriteMyPaperOnCincinnati100% (1)
- Anesthesia and Analgesia in The NICUDocumento19 páginasAnesthesia and Analgesia in The NICUPaulHerreraAún no hay calificaciones
- Pain Management in Infants, Children, AdolescentsDocumento9 páginasPain Management in Infants, Children, AdolescentsمعتزباللهAún no hay calificaciones
- Assesing Pain in Children in The Perioperative SettingDocumento8 páginasAssesing Pain in Children in The Perioperative Settingfuka priesleyAún no hay calificaciones
- Dolor Crónico Infantily FTDocumento13 páginasDolor Crónico Infantily FTmonicaAún no hay calificaciones
- D3kepma2a - Tika Dwi Aprilliani - P17210182044Documento17 páginasD3kepma2a - Tika Dwi Aprilliani - P17210182044mufid dodyAún no hay calificaciones
- Boulkedid 2017Documento11 páginasBoulkedid 2017Ariadna BarretoAún no hay calificaciones
- Literature Review Pain AssessmentDocumento8 páginasLiterature Review Pain Assessmentc5r0xg9z100% (1)
- 4.neonatal Pain ManagementDocumento6 páginas4.neonatal Pain ManagementINGRIT LORENA MONTOYA FERNANDEZAún no hay calificaciones
- Pain Assessment in PediatricDocumento4 páginasPain Assessment in PediatricfitriaAún no hay calificaciones
- 9 Anak (Manajemen Nyeri)Documento7 páginas9 Anak (Manajemen Nyeri)dewiAún no hay calificaciones
- Ger - Leung, Brenda Takeda, Wendy Holec, Victoria. (2018)Documento8 páginasGer - Leung, Brenda Takeda, Wendy Holec, Victoria. (2018)Rafael CostaAún no hay calificaciones
- Tingkat NyeriDocumento9 páginasTingkat NyeriMiaAún no hay calificaciones
- Pain Management in ChildrenDocumento9 páginasPain Management in ChildrenNASLY YERALDINE ZAPATA CATAÑOAún no hay calificaciones
- 2020 - Linical Implications of Unmanaged Needle-InsertionDocumento6 páginas2020 - Linical Implications of Unmanaged Needle-InsertionPoliana carmonaAún no hay calificaciones
- Nonpharmacologic Intervention On The Prevention of Pain and Anxiety During Pediatric Dental Care: A Systematic ReviewDocumento11 páginasNonpharmacologic Intervention On The Prevention of Pain and Anxiety During Pediatric Dental Care: A Systematic ReviewJorge Luis Ramos MaqueraAún no hay calificaciones
- NursingDocumento24 páginasNursingPrita LestariAún no hay calificaciones
- Research Paper On PainDocumento8 páginasResearch Paper On Painyjtpbivhf100% (1)
- BP PainmanagementDocumento24 páginasBP PainmanagementbaridinoAún no hay calificaciones
- Abdominal Pain 3Documento11 páginasAbdominal Pain 3Alejandra Cienfuegos LopezAún no hay calificaciones
- Practical Treatment Options for Chronic Pain in Children and Adolescents: An Interdisciplinary Therapy ManualDe EverandPractical Treatment Options for Chronic Pain in Children and Adolescents: An Interdisciplinary Therapy ManualAún no hay calificaciones
- Therapist's Guide to Pediatric Affect and Behavior RegulationDe EverandTherapist's Guide to Pediatric Affect and Behavior RegulationAún no hay calificaciones
- Application Form - Scholarship 2015-2016Documento15 páginasApplication Form - Scholarship 2015-2016Abdul Khalik AssufiAún no hay calificaciones
- Tugas Bing 2Documento2 páginasTugas Bing 2Hanifa Nur AfifahAún no hay calificaciones
- Contoh Soal Uji Kompetensi Keperawatan KomunitasDocumento39 páginasContoh Soal Uji Kompetensi Keperawatan KomunitasUmairohSetengahTiga67% (3)
- Skema Rantai Pemutus InfeksiDocumento1 páginaSkema Rantai Pemutus InfeksiHanifa Nur AfifahAún no hay calificaciones
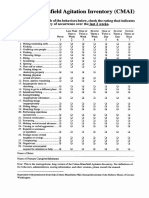
- 738 CMAI Scale5b25d PDFDocumento1 página738 CMAI Scale5b25d PDFShes-Jap Te NdryshmeAún no hay calificaciones
- Name: Vicky Dian Febriani NIM: I31110031Documento3 páginasName: Vicky Dian Febriani NIM: I31110031Hanifa Nur AfifahAún no hay calificaciones
- KozierhDocumento1 páginaKozierhHanifa Nur AfifahAún no hay calificaciones
- Humor TherapyDocumento9 páginasHumor TherapyHanifa Nur AfifahAún no hay calificaciones
- Daftar PustakaDocumento1 páginaDaftar PustakaHanifa Nur AfifahAún no hay calificaciones
- Hospital Anxiety and Depression Scale (HADS)Documento5 páginasHospital Anxiety and Depression Scale (HADS)BahRunAún no hay calificaciones
- Dyspnea Management in Early-Stage Lung Cancer: A Palliative PerspectiveDocumento9 páginasDyspnea Management in Early-Stage Lung Cancer: A Palliative PerspectiveHanifa Nur AfifahAún no hay calificaciones
- Emerging Concepts in The Diagnosis and Treatment of Patients With Undifferentiated AngioedemaDocumento13 páginasEmerging Concepts in The Diagnosis and Treatment of Patients With Undifferentiated AngioedemaHanifa Nur AfifahAún no hay calificaciones
- 1hDocumento7 páginas1hHanifa Nur AfifahAún no hay calificaciones
- KozierhDocumento1 páginaKozierhHanifa Nur AfifahAún no hay calificaciones
- Dyspnea Management in Early-Stage Lung Cancer: A Palliative PerspectiveDocumento9 páginasDyspnea Management in Early-Stage Lung Cancer: A Palliative PerspectiveHanifa Nur AfifahAún no hay calificaciones
- KozierhDocumento1 páginaKozierhHanifa Nur AfifahAún no hay calificaciones
- Pharmanovaprice List July ExcelDocumento13 páginasPharmanovaprice List July ExcelSagar GargAún no hay calificaciones
- OxyContin (Oxycodone) MundipharmaDocumento15 páginasOxyContin (Oxycodone) MundipharmaRayzal AdamAún no hay calificaciones
- Chronic Pain SAQ'sDocumento52 páginasChronic Pain SAQ'sNaser AhmedAún no hay calificaciones
- There Are Different Types of PainDocumento2 páginasThere Are Different Types of PainMary Scarlette CenaAún no hay calificaciones
- Pain and Perioperative NursingDocumento28 páginasPain and Perioperative NursingRonica MendozaAún no hay calificaciones
- Pain ManagementDocumento175 páginasPain ManagementGusni FitriAún no hay calificaciones
- Effectiveness of Acupuncture For Pain Control After Cesarean Delivery A Randomized Clinical TrialDocumento13 páginasEffectiveness of Acupuncture For Pain Control After Cesarean Delivery A Randomized Clinical TrialgigicarvajalAún no hay calificaciones
- 1ZH Anterior RhinosDocumento50 páginas1ZH Anterior RhinosAizat ZulkifliAún no hay calificaciones
- Prescribing in Patients With Liver Disease: Rakesh K TandonDocumento4 páginasPrescribing in Patients With Liver Disease: Rakesh K Tandonjoydeep chakrabortyAún no hay calificaciones
- Raja Srinivas CVDocumento32 páginasRaja Srinivas CVEvanora JavaAún no hay calificaciones
- Andhika Rezeky Gunawan - Tugas FarmakoDocumento4 páginasAndhika Rezeky Gunawan - Tugas FarmakoAndhika gunawanAún no hay calificaciones
- Pfizer Canada Inc., & Warner-Lambert Company V Pharmascience Inc. & The Minister of HealthDocumento86 páginasPfizer Canada Inc., & Warner-Lambert Company V Pharmascience Inc. & The Minister of HealthIlyaAún no hay calificaciones
- Opioid Analgesics - A 2018 Update: SA Pharmaceutical Journal January 2018Documento8 páginasOpioid Analgesics - A 2018 Update: SA Pharmaceutical Journal January 2018Prudhvi Sai NidadavoluAún no hay calificaciones
- CASE FOUR: Bitter Pill: Collect Your Tools and Head To The Crime SceneDocumento5 páginasCASE FOUR: Bitter Pill: Collect Your Tools and Head To The Crime SceneDiegoAún no hay calificaciones
- Chapter 5Documento52 páginasChapter 5Daily BreadAún no hay calificaciones
- Evaluation and Management of Pain in ChildrenDocumento13 páginasEvaluation and Management of Pain in ChildrenOlga MoţpanAún no hay calificaciones
- Nursing Care PlanDocumento10 páginasNursing Care PlanIsabelle Madrid100% (1)
- Study of Analgesic Activity of Cow Urine and Its Distillate by Rat-Tail Immersion MethodDocumento2 páginasStudy of Analgesic Activity of Cow Urine and Its Distillate by Rat-Tail Immersion MethodpatelsspAún no hay calificaciones
- Effect of Foot Massages On Postpartum Comfort And.6Documento10 páginasEffect of Foot Massages On Postpartum Comfort And.6Siti lestarinurhamidahAún no hay calificaciones
- Delivery Room Drug StudyDocumento9 páginasDelivery Room Drug Studymacel sibayan100% (9)
- NsaidDocumento29 páginasNsaidAnonymous vMjb3lQOPoAún no hay calificaciones
- List of Drugs Pharmacology 2Documento13 páginasList of Drugs Pharmacology 2Maisarah Ab SamadAún no hay calificaciones
- GROUP4 - CLUSTER1 - IIID - NCP Stomach CancerDocumento2 páginasGROUP4 - CLUSTER1 - IIID - NCP Stomach CancerJulienne Pucan0% (1)
- Controversiesindental Traumatology: Orrett E. OgleDocumento15 páginasControversiesindental Traumatology: Orrett E. OglechannadrasmaAún no hay calificaciones
- Opioids AutacoidsDocumento22 páginasOpioids AutacoidsSiddharth Anand80% (5)
- ESCEO Algoritmo Manejo OADocumento9 páginasESCEO Algoritmo Manejo OAMarco LenzAún no hay calificaciones
- Unit 5 SuppositoriesDocumento47 páginasUnit 5 SuppositoriesAsif AAún no hay calificaciones