También podría gustarte
- Achalasia: Proximal Dysphagia Due To Neuromuscular Cause Distal Dysphagia Due To Mechanical ObstructionDocumento10 páginasAchalasia: Proximal Dysphagia Due To Neuromuscular Cause Distal Dysphagia Due To Mechanical ObstructionJohnpeter EsporlasAún no hay calificaciones
- B. The Contrecoup Injury Occurs Directly Opposite To The Point of ImpactDocumento4 páginasB. The Contrecoup Injury Occurs Directly Opposite To The Point of ImpactJohnpeter EsporlasAún no hay calificaciones
- Assistive Devices RealDocumento3 páginasAssistive Devices RealJohnpeter EsporlasAún no hay calificaciones
- Postpolio SyndromeDocumento3 páginasPostpolio SyndromeJohnpeter Esporlas100% (1)
- Electrotherapy Parameters For Grand PraxDocumento3 páginasElectrotherapy Parameters For Grand PraxJohnpeter EsporlasAún no hay calificaciones
- Amyotrophic Lateral SclerosisDocumento3 páginasAmyotrophic Lateral SclerosisJohnpeter EsporlasAún no hay calificaciones
- Mes 3Documento4 páginasMes 3Johnpeter EsporlasAún no hay calificaciones
- ReviewDocumento10 páginasReviewJohnpeter EsporlasAún no hay calificaciones
- Is There Anything Left to Trust? - 40-character for document on trusting the BibleDocumento28 páginasIs There Anything Left to Trust? - 40-character for document on trusting the BibleJohnpeter EsporlasAún no hay calificaciones
- Parables of Jesus ChristDocumento4 páginasParables of Jesus ChristJohnpeter EsporlasAún no hay calificaciones
- Bell's PalsyDocumento9 páginasBell's PalsyJohnpeter EsporlasAún no hay calificaciones
- Introduction To PharmacologyDocumento6 páginasIntroduction To PharmacologyJohnpeter EsporlasAún no hay calificaciones
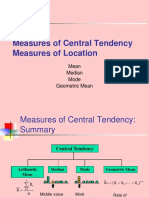
- Central TendencyDocumento25 páginasCentral TendencyJohnpeter EsporlasAún no hay calificaciones
- TEP 2 Syllabus and Course Overviews for Physiotherapy ModulesDocumento2 páginasTEP 2 Syllabus and Course Overviews for Physiotherapy ModulesJohnpeter EsporlasAún no hay calificaciones
- Pediatric Milestones Age Gross Motor Fine Motor Personal/Social Speech and LanguageDocumento3 páginasPediatric Milestones Age Gross Motor Fine Motor Personal/Social Speech and LanguageJohnpeter EsporlasAún no hay calificaciones
- Cardiovascular RehabilitationDocumento5 páginasCardiovascular RehabilitationJohnpeter EsporlasAún no hay calificaciones
- Tep 11 Reflexes PrintoutDocumento2 páginasTep 11 Reflexes PrintoutJohnpeter EsporlasAún no hay calificaciones
- KneeDocumento14 páginasKneeJohnpeter Esporlas100% (1)
- Atlas of Digestive SystemDocumento3 páginasAtlas of Digestive SystemJohnpeter EsporlasAún no hay calificaciones
- Patient Survey Results Guide Practice ImprovementsDocumento6 páginasPatient Survey Results Guide Practice ImprovementsJohnpeter EsporlasAún no hay calificaciones
- SHOULDER PAIN AND INJURY GUIDEDocumento7 páginasSHOULDER PAIN AND INJURY GUIDEJohnpeter EsporlasAún no hay calificaciones
- Chapter 12Documento22 páginasChapter 12John EmmanuelAún no hay calificaciones
- CVA - Compilation of All BooksDocumento4 páginasCVA - Compilation of All BooksJohnpeter EsporlasAún no hay calificaciones
- Neuroanatomy Pictures Part 2 - WaxmanDocumento6 páginasNeuroanatomy Pictures Part 2 - WaxmanJohnpeter EsporlasAún no hay calificaciones
- Effects of Prolonged Immobilization on the Musculoskeletal SystemDocumento14 páginasEffects of Prolonged Immobilization on the Musculoskeletal SystemJohnpeter EsporlasAún no hay calificaciones
- Normal Body TemperaturesDocumento5 páginasNormal Body TemperaturesJohnpeter EsporlasAún no hay calificaciones
- CBR Topic Outline 2017-2018Documento3 páginasCBR Topic Outline 2017-2018Johnpeter EsporlasAún no hay calificaciones
- Anthropometric SDocumento3 páginasAnthropometric SJohnpeter EsporlasAún no hay calificaciones
- Down SyndromeDocumento2 páginasDown SyndromeJohnpeter EsporlasAún no hay calificaciones
- Etiology, Epidemiology & Differential Diagnosis For CADDocumento9 páginasEtiology, Epidemiology & Differential Diagnosis For CADJohnpeter EsporlasAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Index - 8.8 Eu PharmDocumento56 páginasIndex - 8.8 Eu PharmAnonymous iOYpj92Aún no hay calificaciones
- PMLS - Definition of Curriculum and Overview of CoursesDocumento5 páginasPMLS - Definition of Curriculum and Overview of CoursesVine OrtegaAún no hay calificaciones
- Qualitative Platelet DisordersDocumento5 páginasQualitative Platelet DisordersChristyl JoAún no hay calificaciones
- Fped 09 591052Documento6 páginasFped 09 591052husna fitriaAún no hay calificaciones
- CARE PLAN On HyponatremiaDocumento35 páginasCARE PLAN On Hyponatremia2020 MSc bhuvaneswari 05Aún no hay calificaciones
- HaematologyDocumento68 páginasHaematologytapoolnoAún no hay calificaciones
- Activated Partial Thromboplastin Time (aPTT) Mr. Khaled AlzatariDocumento16 páginasActivated Partial Thromboplastin Time (aPTT) Mr. Khaled AlzatariKhaled ZatariAún no hay calificaciones
- Fulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakyDocumento108 páginasFulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakypadmaAún no hay calificaciones
- Blood Trasnfusions 1Documento7 páginasBlood Trasnfusions 1Silvia RodríguezAún no hay calificaciones
- 2023 Therapeutic Plasma ExchangeDocumento18 páginas2023 Therapeutic Plasma ExchangeJesus PlanellesAún no hay calificaciones
- Blood Transfusion & ComponentsDocumento56 páginasBlood Transfusion & Componentsadithya polavarapuAún no hay calificaciones
- HEMAREV Merged PDFDocumento120 páginasHEMAREV Merged PDFMae BaechuAún no hay calificaciones
- Anticoagulants and Antiplatelet AgentsDocumento4 páginasAnticoagulants and Antiplatelet AgentsMark Russel Sean LealAún no hay calificaciones
- Damage Control ResuscitationDocumento32 páginasDamage Control Resuscitationrima oktariniAún no hay calificaciones
- Blood Coagulation 2011Documento64 páginasBlood Coagulation 2011azizAún no hay calificaciones
- Heparin and WarfarinDocumento2 páginasHeparin and WarfarinBaeyer100% (1)
- Blood Clotting Mechanisms and Thrombolytic TherapyDocumento3 páginasBlood Clotting Mechanisms and Thrombolytic TherapyLindsey SimmonsAún no hay calificaciones
- Technothrombin TGA Triggers ML-00-00293REV01Documento8 páginasTechnothrombin TGA Triggers ML-00-00293REV01myafiaAún no hay calificaciones
- Combined HemaDocumento28 páginasCombined HemaViena Mae MaglupayAún no hay calificaciones
- THROMBOPHLEBITISDocumento25 páginasTHROMBOPHLEBITISCamille Maluenda - Tan100% (2)
- Abstracts CopenhagenDocumento127 páginasAbstracts CopenhagenPisica ZmeuAún no hay calificaciones
- MCQ'S in Pharmacology Wid AnswersDocumento18 páginasMCQ'S in Pharmacology Wid Answersapi-1991639975% (4)
- Paraneoplastic Syndromes: Dennis B. BaileyDocumento15 páginasParaneoplastic Syndromes: Dennis B. BaileyegagusmelaAún no hay calificaciones
- Disorders of LeukocytesDocumento30 páginasDisorders of LeukocytesLaura Daniela MurilloAún no hay calificaciones
- Polytrauma Jacques Duranteau PDFDocumento48 páginasPolytrauma Jacques Duranteau PDFMarcelo MercadoAún no hay calificaciones
- PDF Copy Haematology Laboratory Manual Cls 241 PDFDocumento70 páginasPDF Copy Haematology Laboratory Manual Cls 241 PDFKahina Ould TalebAún no hay calificaciones
- Direct Oral Anticoagulants From Pharmacology To Clinical PracticeDocumento283 páginasDirect Oral Anticoagulants From Pharmacology To Clinical PracticesunhaolanAún no hay calificaciones
- Sickle Cell AnemiaDocumento7 páginasSickle Cell AnemiaJuma AwarAún no hay calificaciones
- 2934 Hemochron ManualDocumento32 páginas2934 Hemochron ManualFrank QuitianAún no hay calificaciones
- Rusun Medical Leader in Hemostatic ProductsDocumento33 páginasRusun Medical Leader in Hemostatic ProductsCalvin hobbesAún no hay calificaciones