También podría gustarte
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Ddec III-IV Single Ecm Troubleshooting GuideDocumento12 páginasDdec III-IV Single Ecm Troubleshooting GuideLuis JesusAún no hay calificaciones
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- DF 2-8 ManualDocumento113 páginasDF 2-8 Manualamin_bravoAún no hay calificaciones
- Module - 5: Power AmplifiersDocumento58 páginasModule - 5: Power AmplifiersSILPA AJITH100% (2)
- TAs Amp AudioDocumento65 páginasTAs Amp Audiocarlos pachecoAún no hay calificaciones
- Datex Capnomac Ultima Monitor - Service Manual PDFDocumento232 páginasDatex Capnomac Ultima Monitor - Service Manual PDFFernandoAún no hay calificaciones
- Wireless E Notice BoardDocumento5 páginasWireless E Notice Board1200miqaelAún no hay calificaciones
- Centralized Automated Network OptimizationDocumento2 páginasCentralized Automated Network OptimizationNguyen Dang KhanhAún no hay calificaciones
- Product Information Sheet: Customer Communication Module (CCM)Documento2 páginasProduct Information Sheet: Customer Communication Module (CCM)polish22Aún no hay calificaciones
- Digital Tachometer Using Arduino Plus Motor Speed Control. Circuit Diagram and ProgramDocumento12 páginasDigital Tachometer Using Arduino Plus Motor Speed Control. Circuit Diagram and ProgramtummalapaliraviAún no hay calificaciones
- THE 8051 MICROCONTROLLERDocumento49 páginasTHE 8051 MICROCONTROLLERSabuj Ahmed100% (1)
- Dpa Iii Plus and Dpa Ii Plus Quick Start Guide: A. Connecting The DPADocumento2 páginasDpa Iii Plus and Dpa Ii Plus Quick Start Guide: A. Connecting The DPAJoffre Lautaro Benavides SeminarioAún no hay calificaciones
- DekTec DTE-3137Documento7 páginasDekTec DTE-3137Alexander WieseAún no hay calificaciones
- Construct ADAT Sync CableDocumento3 páginasConstruct ADAT Sync CableArtist RecordingAún no hay calificaciones
- P150EM/ P151EM1 Service ManualDocumento124 páginasP150EM/ P151EM1 Service Manualsmooky1980Aún no hay calificaciones
- XK3118T1 Operation ManualDocumento10 páginasXK3118T1 Operation ManualGerardo RodriguezAún no hay calificaciones
- Trident TDA10071 Brief 10002ADocumento2 páginasTrident TDA10071 Brief 10002AmalinnoiAún no hay calificaciones
- Configuracion SelectorDocumento5 páginasConfiguracion SelectorpatricioAún no hay calificaciones
- Why you may get less than promised Internet speeds despite high speed plansDocumento2 páginasWhy you may get less than promised Internet speeds despite high speed plansramakant_soni1988Aún no hay calificaciones
- Wall Box 1 Socket Type 2 Type 2 1P+N+E 32A 230V 7,4kW 32A 230V 1P+N+E IP55 IK08Documento2 páginasWall Box 1 Socket Type 2 Type 2 1P+N+E 32A 230V 7,4kW 32A 230V 1P+N+E IP55 IK08viorel8ungurianuAún no hay calificaciones
- MBI Driver IC For LED Display ScreenDocumento14 páginasMBI Driver IC For LED Display ScreenAcido CinicoAún no hay calificaciones
- E1509-Tls Calc Table - Not TemplateDocumento63 páginasE1509-Tls Calc Table - Not TemplateDanielAún no hay calificaciones
- Multi-Network Combiner: Product Code: PW-SMOC-10I4O-ADocumento14 páginasMulti-Network Combiner: Product Code: PW-SMOC-10I4O-AsetiadhyAún no hay calificaciones
- Stress Meter Mini ProjectDocumento23 páginasStress Meter Mini ProjectCheruku AbhilashAún no hay calificaciones
- Lenovo V130 20IGM AIO SpecDocumento7 páginasLenovo V130 20IGM AIO SpecYimele SeraphimAún no hay calificaciones
- Objective Measurement of The Speech Privacy Provided by A Closed RoomDocumento8 páginasObjective Measurement of The Speech Privacy Provided by A Closed RoomAhmad Zubair RasulyAún no hay calificaciones
- 2007 Nonis TCAS CML Divider DesignDocumento10 páginas2007 Nonis TCAS CML Divider DesignDavidAún no hay calificaciones
- Migration To Softswitch Solutions: Paul Brittain Product Manager, MetaswitchDocumento13 páginasMigration To Softswitch Solutions: Paul Brittain Product Manager, Metaswitchnguyenductanhn85Aún no hay calificaciones
- ZK SAMpDocumento2 páginasZK SAMpEddy FungAún no hay calificaciones
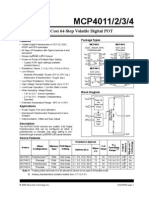
- MCP4011 Digital PotDocumento60 páginasMCP4011 Digital Potundes100% (1)
- Wolf Richarrd VISH212-IDocumento29 páginasWolf Richarrd VISH212-ISwami Meera100% (1)