También podría gustarte
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsDe EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsCalificación: 4.5 de 5 estrellas4.5/5 (13)
- 2015-Wade Financial DisclosureDocumento7 páginas2015-Wade Financial DisclosuredavidsirotaAún no hay calificaciones
- Gina McCarthy Financial DisclosuresDocumento49 páginasGina McCarthy Financial DisclosuresLachlan MarkayAún no hay calificaciones
- IA-AINP Family Sponsorship AffidavitDocumento5 páginasIA-AINP Family Sponsorship AffidavitHasmukhAún no hay calificaciones
- WPS-190338676 613letDocumento6 páginasWPS-190338676 613letDennis KingAún no hay calificaciones
- TCF Equipment Finance Credit AppDocumento1 páginaTCF Equipment Finance Credit Appjasonparker80Aún no hay calificaciones
- ALAN-I GOLDBERG Initial Disclosure 2015 06-17-5581e6768e791Documento77 páginasALAN-I GOLDBERG Initial Disclosure 2015 06-17-5581e6768e791ALAN I GOLDBERGAún no hay calificaciones
- Answer All Items: Fill in With Typewriter or Print in Block Letters in Ink.Documento4 páginasAnswer All Items: Fill in With Typewriter or Print in Block Letters in Ink.taarkikaAún no hay calificaciones
- Application For Housing Assistance: Use This Form To Apply For Social Housing Assistance in New South WalesDocumento18 páginasApplication For Housing Assistance: Use This Form To Apply For Social Housing Assistance in New South WalesVincent HardyAún no hay calificaciones
- Insurance Beneficiary Payment DetailsDocumento1 páginaInsurance Beneficiary Payment DetailsAnonymous Ebd2V9Aún no hay calificaciones
- Application Instructions for License and Permit BondsDocumento9 páginasApplication Instructions for License and Permit Bondslearnlaw.us8393Aún no hay calificaciones
- Form 1 - Patient Registration InformationDocumento1 páginaForm 1 - Patient Registration Informationapi-262575736Aún no hay calificaciones
- Medicaid ApplicationDocumento27 páginasMedicaid ApplicationIndiana Family to Family100% (1)
- Application Business Loan SHORT FORM PDFDocumento2 páginasApplication Business Loan SHORT FORM PDFGeorgiMoskeyMarinoAún no hay calificaciones
- Onondaga County Legislator Timothy Burtis Financial Disclosure 2015Documento3 páginasOnondaga County Legislator Timothy Burtis Financial Disclosure 2015Michelle BreidenbachAún no hay calificaciones
- Candidate Info Sheet SummaryDocumento4 páginasCandidate Info Sheet SummaryRiyaz AhmadAún no hay calificaciones
- Support Payment Credit Information Sheet: Return Completed Form (S) ToDocumento6 páginasSupport Payment Credit Information Sheet: Return Completed Form (S) ToMaria EAún no hay calificaciones
- DE2501 (1) CA DisablityDocumento5 páginasDE2501 (1) CA DisablitysteveAún no hay calificaciones
- Arpdf RRDocumento9 páginasArpdf RRsidewalksurfer505Aún no hay calificaciones
- Blue Card Volunteer FormDocumento4 páginasBlue Card Volunteer FormWednesday FelodeseAún no hay calificaciones
- Notice of Conditional AcceptanceDocumento11 páginasNotice of Conditional AcceptanceMichael Kovach100% (12)
- 2018 Statement of Financial DisclosureDocumento4 páginas2018 Statement of Financial DisclosureAnnie AndersenAún no hay calificaciones
- Application For Financial Assistance For Undergraduate Studies in 2013Documento6 páginasApplication For Financial Assistance For Undergraduate Studies in 2013211505006Aún no hay calificaciones
- Ic 1Documento6 páginasIc 1amjadbonusAún no hay calificaciones
- Conditional AcceptanceDocumento9 páginasConditional AcceptanceSpike Lee92% (12)
- What Should IKnowDocumento8 páginasWhat Should IKnowJessica MartinAún no hay calificaciones
- Ann18743 (717) 68706Documento10 páginasAnn18743 (717) 68706GustaveFlaubertAún no hay calificaciones
- ALBIS 2012 Contribution FormDocumento1 páginaALBIS 2012 Contribution Formjames_albis5632Aún no hay calificaciones
- New Credit AppDocumento5 páginasNew Credit Appapi-282795606Aún no hay calificaciones
- COMMERCIAL LOAN Application - Full or Stated DocumentationDocumento5 páginasCOMMERCIAL LOAN Application - Full or Stated DocumentationJulio Cesar NavasAún no hay calificaciones
- Affidavit of Support for Indian Cousin Kuldeep SinghDocumento2 páginasAffidavit of Support for Indian Cousin Kuldeep SinghAnit SharmaAún no hay calificaciones
- Credit ApplicationDocumento3 páginasCredit ApplicationShelbyElliottAún no hay calificaciones
- PFD 317 140463603Documento1 páginaPFD 317 140463603kcc2012Aún no hay calificaciones
- NQ Non-Spouse Rind - 0080Documento5 páginasNQ Non-Spouse Rind - 0080Alexander HerbertAún no hay calificaciones
- Affidavit I-864 Under213ADocumento8 páginasAffidavit I-864 Under213AMariama DiaoAún no hay calificaciones
- Your Background Order: Dob: SSNDocumento6 páginasYour Background Order: Dob: SSNDed MarozAún no hay calificaciones
- N0 SSN For BAnk AccountDocumento6 páginasN0 SSN For BAnk AccountColton Robert100% (14)
- 2016 CEP Donation FormA Tillett4CTDocumento2 páginas2016 CEP Donation FormA Tillett4CTtillett4ctAún no hay calificaciones
- Affidavit of Support Form I-134 ExplainedDocumento2 páginasAffidavit of Support Form I-134 ExplainedOscar MartinezAún no hay calificaciones
- CWCS Founding DocumentsDocumento98 páginasCWCS Founding DocumentsWilliamsburg GreenpointAún no hay calificaciones
- rd1980-21 2-2013Documento4 páginasrd1980-21 2-2013api-196037134Aún no hay calificaciones
- ITT Tech Bankruptcy FilingDocumento11 páginasITT Tech Bankruptcy FilingMallory DuncanAún no hay calificaciones
- Bank Version Personal Financial StatementDocumento9 páginasBank Version Personal Financial StatementJk McCrea100% (1)
- Purok Santol Celdran Village, Camague Iligan CityDocumento5 páginasPurok Santol Celdran Village, Camague Iligan CityAubrey CaballeroAún no hay calificaciones
- Mail in Donation FormA Tillett4CT PO Box 602Documento2 páginasMail in Donation FormA Tillett4CT PO Box 602tillett4ctAún no hay calificaciones
- Applying For A Departing Australia Superannuation Payment: Instructions and Form For Temporary ResidentsDocumento10 páginasApplying For A Departing Australia Superannuation Payment: Instructions and Form For Temporary ResidentsnickECEAún no hay calificaciones
- Michael D Nieves - TransUnion Personal Credit Report - 20140730Documento5 páginasMichael D Nieves - TransUnion Personal Credit Report - 20140730chfthegodAún no hay calificaciones
- Independent ContractDocumento3 páginasIndependent Contractapi-11899786Aún no hay calificaciones
- Request For Taxpayer Identification Number and CertificationDocumento1 páginaRequest For Taxpayer Identification Number and CertificationJude Thomas SmithAún no hay calificaciones
- Affidavit of Assets and Liabilities For Non-Agrarian DeponentsDocumento4 páginasAffidavit of Assets and Liabilities For Non-Agrarian Deponentsensymte50Aún no hay calificaciones
- PRE-PAID LEGAL SERVICES APPLICATIONDocumento2 páginasPRE-PAID LEGAL SERVICES APPLICATIONHunter GrayAún no hay calificaciones
- Request Banks To Follow UCC PROOF OF CLAIMDocumento4 páginasRequest Banks To Follow UCC PROOF OF CLAIMZIONCREDITGROUP100% (19)
- Statement of Economic InterestDocumento33 páginasStatement of Economic InterestProgressVAAún no hay calificaciones
- Application Form: Tata Aia Life Insurance Company LimitedDocumento6 páginasApplication Form: Tata Aia Life Insurance Company LimitedpritamAún no hay calificaciones
- Request to Stop Tax Withholding AffidavitDocumento17 páginasRequest to Stop Tax Withholding AffidavitBar RiAún no hay calificaciones
- Inaugural Ball and FormsDocumento3 páginasInaugural Ball and FormsThe Valley IndyAún no hay calificaciones
- Federal Reserve Language - StimulusDocumento8 páginasFederal Reserve Language - StimulusdavidsirotaAún no hay calificaciones
- Mary Nichols AnnualDocumento15 páginasMary Nichols AnnualdavidsirotaAún no hay calificaciones
- Bernie 2020 Polling MemoDocumento3 páginasBernie 2020 Polling MemodavidsirotaAún no hay calificaciones
- CDPHE ResponseDocumento1 páginaCDPHE ResponsedavidsirotaAún no hay calificaciones
- Daily Poster - Draft Senate Liability LegislationDocumento18 páginasDaily Poster - Draft Senate Liability LegislationdavidsirotaAún no hay calificaciones
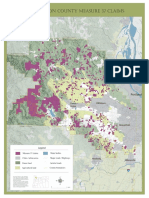
- Clackamas County - Measure 37Documento1 páginaClackamas County - Measure 37davidsirotaAún no hay calificaciones
- Biden Pool Report - 7/20/20Documento3 páginasBiden Pool Report - 7/20/20davidsirota100% (2)
- Mary Nichols - 2018 AnnualDocumento40 páginasMary Nichols - 2018 AnnualdavidsirotaAún no hay calificaciones
- Draft - Senate Emergency StimulusDocumento525 páginasDraft - Senate Emergency Stimulusdavidsirota100% (1)
- Judicial Crisis Network 990 - 2018-2019Documento36 páginasJudicial Crisis Network 990 - 2018-2019davidsirota0% (1)
- KDVR Cease and DesistDocumento2 páginasKDVR Cease and DesistdavidsirotaAún no hay calificaciones
- Memorandum: A. Regulatory Takings Law GenerallyDocumento3 páginasMemorandum: A. Regulatory Takings Law GenerallydavidsirotaAún no hay calificaciones
- Colorado Farm Bureau Letter To Municipal OfficialsDocumento6 páginasColorado Farm Bureau Letter To Municipal OfficialsdavidsirotaAún no hay calificaciones
- Washington County - Measure 37Documento1 páginaWashington County - Measure 37davidsirotaAún no hay calificaciones
- Environmental Groups Request JCOPE InvestigationDocumento7 páginasEnvironmental Groups Request JCOPE InvestigationdavidsirotaAún no hay calificaciones
- Fuller Conflict of Interest Williams Aug18Documento3 páginasFuller Conflict of Interest Williams Aug18City & State NYAún no hay calificaciones
- Williams Co DGA DonationDocumento1 páginaWilliams Co DGA DonationdavidsirotaAún no hay calificaciones
- NY Comptroller Response To Environmental GroupsDocumento2 páginasNY Comptroller Response To Environmental GroupsdavidsirotaAún no hay calificaciones
- Williams Transco DGA DonationDocumento1 páginaWilliams Transco DGA DonationdavidsirotaAún no hay calificaciones
- Colorado Governors Office Agreement - Completed - Signed Governor Hickenlooper PDFDocumento2 páginasColorado Governors Office Agreement - Completed - Signed Governor Hickenlooper PDFdavidsirotaAún no hay calificaciones
- Senate Letter To United AirlinesDocumento5 páginasSenate Letter To United Airlinesdavidsirota100% (2)
- Contract Between Gov. Hickenlooper's Office and Brownstein Hyatt Farber Schreck LLCDocumento4 páginasContract Between Gov. Hickenlooper's Office and Brownstein Hyatt Farber Schreck LLCdavidsirotaAún no hay calificaciones
- Roffman TestimonyDocumento5 páginasRoffman TestimonydavidsirotaAún no hay calificaciones
- Arkema's May 15, 2017 Letter Calling For Repeal of EPA's Chemical Plant Safety RuleDocumento4 páginasArkema's May 15, 2017 Letter Calling For Repeal of EPA's Chemical Plant Safety RuledavidsirotaAún no hay calificaciones
- United Airlines Comments To Federal RegulatorsDocumento41 páginasUnited Airlines Comments To Federal RegulatorsdavidsirotaAún no hay calificaciones
- Third Circuit Appeal - TrumpDocumento33 páginasThird Circuit Appeal - TrumpdavidsirotaAún no hay calificaciones
- Emails From Colorado Gov. John Hickenlooper's OfficeDocumento2 páginasEmails From Colorado Gov. John Hickenlooper's OfficedavidsirotaAún no hay calificaciones
- New Jersey District Court TestimonyDocumento34 páginasNew Jersey District Court TestimonydavidsirotaAún no hay calificaciones
- New Jersey District Court - TrumpDocumento64 páginasNew Jersey District Court - TrumpdavidsirotaAún no hay calificaciones
- Juvenile Justice Welfare ActDocumento9 páginasJuvenile Justice Welfare ActКатрина ШараповаAún no hay calificaciones
- Introduction of ContractDocumento2 páginasIntroduction of ContractNicole AgostoAún no hay calificaciones
- Alejandro C. Almendras, JR., Petitioner, vs. Alexis C. Almendras, RespondentDocumento4 páginasAlejandro C. Almendras, JR., Petitioner, vs. Alexis C. Almendras, RespondentMarianne Shen PetillaAún no hay calificaciones
- Valenzuela vs. CADocumento8 páginasValenzuela vs. CARomy Ian LimAún no hay calificaciones
- 02 Pol Science Mains 2019 PDFDocumento37 páginas02 Pol Science Mains 2019 PDFGoogle UserAún no hay calificaciones
- As 4349.0-2007 Inspection of Buildings General RequirementsDocumento8 páginasAs 4349.0-2007 Inspection of Buildings General RequirementsSAI Global - APACAún no hay calificaciones
- LL 6 - Agoy v. NLRC GR 112096 January 30, 1996Documento11 páginasLL 6 - Agoy v. NLRC GR 112096 January 30, 1996raikha barraAún no hay calificaciones
- Judicial Ethics DigestsDocumento23 páginasJudicial Ethics DigestsJanineAún no hay calificaciones
- 80 Gonzales vs. GJH Land, Inc.Documento6 páginas80 Gonzales vs. GJH Land, Inc.joyeduardoAún no hay calificaciones
- The Muslim Concept of Surrender To God: by Mark NygardDocumento6 páginasThe Muslim Concept of Surrender To God: by Mark NygardmaghniavAún no hay calificaciones
- (U) Daily Activity Report: Marshall DistrictDocumento5 páginas(U) Daily Activity Report: Marshall DistrictFauquier NowAún no hay calificaciones
- Fernando Gallardo V. Juan Borromeo: DecisionDocumento2 páginasFernando Gallardo V. Juan Borromeo: DecisionKRISTINE MAE A. RIVERAAún no hay calificaciones
- Graft and CorruptionDocumento9 páginasGraft and CorruptionMel Jazer CAPEAún no hay calificaciones
- Partition Deed LawRato4Documento3 páginasPartition Deed LawRato4Annai SagayamAún no hay calificaciones
- MPA-Local GovernanceDocumento2 páginasMPA-Local GovernanceRein DrewAún no hay calificaciones
- Akhil Gogoi Judgeme1Documento57 páginasAkhil Gogoi Judgeme1DipeshAún no hay calificaciones
- Bangalisan V Ca G.R. No. 124678 July 31, 1997 Regalado, J.: FactsDocumento1 páginaBangalisan V Ca G.R. No. 124678 July 31, 1997 Regalado, J.: FactsKate GaroAún no hay calificaciones
- E1 SBD4 Declaration of Interest - Issue 1 NT005-2011Documento3 páginasE1 SBD4 Declaration of Interest - Issue 1 NT005-2011Teboho MokhesengAún no hay calificaciones
- Phcci MPC Tacloban Laboratory Cooperative Membership FormDocumento2 páginasPhcci MPC Tacloban Laboratory Cooperative Membership Form88grealtiesAún no hay calificaciones
- Albana V Director of PatentsDocumento1 páginaAlbana V Director of PatentsSJ De GuzmanAún no hay calificaciones
- PROTOCOL Agreement Between Cyprus and PolandDocumento7 páginasPROTOCOL Agreement Between Cyprus and PolandOECD: Organisation for Economic Co-operation and DevelopmentAún no hay calificaciones
- 2008 Canlii 3969Documento13 páginas2008 Canlii 3969LarchmanAún no hay calificaciones
- RTC Rape Case AffidavitDocumento6 páginasRTC Rape Case AffidavitArgie DionioAún no hay calificaciones
- Vfp. Vfpia and The VMDCDocumento28 páginasVfp. Vfpia and The VMDCPrincess Trisha Joy UyAún no hay calificaciones
- TEMN/Pierce Answer and Affirmative Defenses (4!24!14)Documento10 páginasTEMN/Pierce Answer and Affirmative Defenses (4!24!14)smallcapsmarketAún no hay calificaciones
- Articles of IncorporationDocumento4 páginasArticles of IncorporationDenis StevensAún no hay calificaciones
- Art. 1207-1222 Study GuideDocumento3 páginasArt. 1207-1222 Study GuideChristine SuarezAún no hay calificaciones
- Providing Drinking Water to VillagersDocumento14 páginasProviding Drinking Water to VillagersKalpana GundumoluAún no hay calificaciones
- Wfo Policy 2023Documento4 páginasWfo Policy 2023semren khanAún no hay calificaciones
- Attachment A - Letter To Nevada Commission On Judicial DisciplineDocumento4 páginasAttachment A - Letter To Nevada Commission On Judicial DisciplineRiley SnyderAún no hay calificaciones