También podría gustarte
- D - Renal PhysiologyDocumento26 páginasD - Renal PhysiologyMohamad Zekry ZuhairyAún no hay calificaciones
- C - Cardiovascular PhysiologyDocumento61 páginasC - Cardiovascular PhysiologyMohamad Zekry ZuhairyAún no hay calificaciones
- B - Respiratory PhysiologyDocumento73 páginasB - Respiratory PhysiologyMohamad Zekry ZuhairyAún no hay calificaciones
- Rapid Sequence InductionDocumento8 páginasRapid Sequence InductionAngela Mitchelle NyanganAún no hay calificaciones
- Rapid Sequence InductionDocumento8 páginasRapid Sequence InductionAngela Mitchelle NyanganAún no hay calificaciones
- A - Cellular PhysiologyDocumento12 páginasA - Cellular PhysiologyMohamad Zekry ZuhairyAún no hay calificaciones
- Body Fluids & ElectrolytesDocumento26 páginasBody Fluids & ElectrolytesMohamad Zekry Zuhairy100% (1)
- Rapid Sequence InductionDocumento8 páginasRapid Sequence InductionAngela Mitchelle NyanganAún no hay calificaciones
- Rapid Sequence InductionDocumento8 páginasRapid Sequence InductionAngela Mitchelle NyanganAún no hay calificaciones
- Khairyst O Khairy Hafizy Turn 10 Happy BirthdayDocumento3 páginasKhairyst O Khairy Hafizy Turn 10 Happy BirthdayMohamad Zekry ZuhairyAún no hay calificaciones
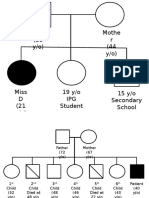
- Geneological ChartDocumento2 páginasGeneological ChartMohamad Zekry ZuhairyAún no hay calificaciones
- Syahmi Mubasyir DiscussionDocumento3 páginasSyahmi Mubasyir DiscussionMohamad Zekry ZuhairyAún no hay calificaciones
- Table15 TypesofHazardDocumento1 páginaTable15 TypesofHazardJackie HwangAún no hay calificaciones
- Endometrial CADocumento74 páginasEndometrial CAMohamad Zekry ZuhairyAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Example Personal StatementsDocumento22 páginasExample Personal Statementsstarblue265100% (1)
- Family Case Study For HydrocephalusDocumento9 páginasFamily Case Study For HydrocephalusjaegergranAún no hay calificaciones
- Community Health NursingDocumento60 páginasCommunity Health NursingDthird Mendoza Claudio100% (2)
- AFT ManualDocumento58 páginasAFT ManualHodaya Ben Shachar50% (2)
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDocumento4 páginasIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsNag Sai NarahariAún no hay calificaciones
- Anxiety Disorder - Module 2 AssignmentDocumento5 páginasAnxiety Disorder - Module 2 Assignmentapi-302174538Aún no hay calificaciones
- Unit 3Documento19 páginasUnit 3deepakAún no hay calificaciones
- BB Summer07 Sleep FinalDocumento2 páginasBB Summer07 Sleep FinalbernicetsyAún no hay calificaciones
- Ultimate Juice Reboot e Book Content 3 D NewDocumento52 páginasUltimate Juice Reboot e Book Content 3 D NewVishalakshi PidaparthiAún no hay calificaciones
- Students Worksheet 9 English For Nursing - Corona Virus Covid-19Documento5 páginasStudents Worksheet 9 English For Nursing - Corona Virus Covid-19Ihat SholihatAún no hay calificaciones
- Alternative Medicine Research Paper RDDocumento7 páginasAlternative Medicine Research Paper RDapi-287616822Aún no hay calificaciones
- Prevention and ControlDocumento2 páginasPrevention and ControlCloue Faye I. BasalloAún no hay calificaciones
- Barriesr in Oral Health CareDocumento2 páginasBarriesr in Oral Health CareRisana RahoofAún no hay calificaciones
- Virginia Henderson's Need Based Theory and Practice ImplicationsDocumento30 páginasVirginia Henderson's Need Based Theory and Practice ImplicationsSadia NadeemAún no hay calificaciones
- KW 15 AbstractsDocumento1129 páginasKW 15 AbstractsShloime-Batsheva Dalezman100% (1)
- Senior Citizen InterviewDocumento4 páginasSenior Citizen Interviewapi-559308608Aún no hay calificaciones
- LIFE INSURANCE JUVENILE MEDICAL FORMDocumento2 páginasLIFE INSURANCE JUVENILE MEDICAL FORMHemant JhaAún no hay calificaciones
- RPT Science Form 2 2023Documento22 páginasRPT Science Form 2 2023peisuanyapAún no hay calificaciones
- Four FacetsDocumento2 páginasFour FacetsJo Hn VengzAún no hay calificaciones
- PMDC Curriculum 2011 PDFDocumento170 páginasPMDC Curriculum 2011 PDFRao Rizwan ShakoorAún no hay calificaciones
- Community Diagnosis FinalDocumento116 páginasCommunity Diagnosis FinalAriane Ballaret75% (8)
- Gesp Forms Sy 2022-2023 - 11302022Documento64 páginasGesp Forms Sy 2022-2023 - 11302022MERY JEAN CATACUTANAún no hay calificaciones
- Diabetic Self-Care Knowledge and Associated Factors Among Adult Diabetes Mellitus Patients On Follow-Up Care at North Shewa Zone Government Hospitals, Oromia Region, Ethiopia, 2020Documento9 páginasDiabetic Self-Care Knowledge and Associated Factors Among Adult Diabetes Mellitus Patients On Follow-Up Care at North Shewa Zone Government Hospitals, Oromia Region, Ethiopia, 2020MAHESH KOUJALAGIAún no hay calificaciones
- Hippocrates in ContextDocumento540 páginasHippocrates in ContextBaruch Von PankäkeAún no hay calificaciones
- Metaphors of PainDocumento16 páginasMetaphors of PainIvana GolubovićAún no hay calificaciones
- WHO / OMS FWC MCA 17.05 EngDocumento44 páginasWHO / OMS FWC MCA 17.05 EngsofiabloemAún no hay calificaciones
- Relationship Between Diet and Stress Levels To Recurrence of Gastritis in The Tarok Puskesmas Work AreaDocumento10 páginasRelationship Between Diet and Stress Levels To Recurrence of Gastritis in The Tarok Puskesmas Work AreaApriyanti BadjiserAún no hay calificaciones
- Intervention-Plan - Grade 10 2019-2020Documento8 páginasIntervention-Plan - Grade 10 2019-2020Cloue Faye I. Basallo100% (1)
- The Precede/Proceed Model: 1. OriginatorsDocumento7 páginasThe Precede/Proceed Model: 1. OriginatorsdrhafizsameeAún no hay calificaciones
- The Impact of Physical Activities On The Health of AdultsDocumento12 páginasThe Impact of Physical Activities On The Health of AdultsJUNAID AHMEDAún no hay calificaciones