También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Analysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsDocumento7 páginasAnalysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsFabian Esteban SubiabreAún no hay calificaciones
- Antagonistas de Los Receptores NMDA Dolor CrónicoDocumento13 páginasAntagonistas de Los Receptores NMDA Dolor CrónicoMario Viazcan CarbajalAún no hay calificaciones
- Analysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsDocumento7 páginasAnalysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsFabian Esteban SubiabreAún no hay calificaciones
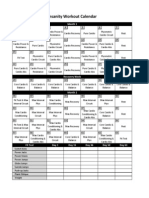
- Cronograma InsanityDocumento1 páginaCronograma InsanityCatherine EcheverryAún no hay calificaciones
- 1984 Early Physiotherapy in The Treatment of Spastic DiplegiaDocumento7 páginas1984 Early Physiotherapy in The Treatment of Spastic DiplegiaFabian Esteban SubiabreAún no hay calificaciones
- Roberto Merletti, Multi Channel Surface EMG For The Non Invasive Assessment of The Anal Sphincter Muscle 2004 Digestion PortoDocumento26 páginasRoberto Merletti, Multi Channel Surface EMG For The Non Invasive Assessment of The Anal Sphincter Muscle 2004 Digestion PortoFabian Esteban SubiabreAún no hay calificaciones
- NAVA HypoventilationDocumento3 páginasNAVA HypoventilationFabian Esteban SubiabreAún no hay calificaciones
- Ooool - Biomecanica Craneo - Cervical y ATMDocumento30 páginasOoool - Biomecanica Craneo - Cervical y ATMFabian Esteban SubiabreAún no hay calificaciones
- Deluca Surface Electromyography Detection&RecordingDocumento10 páginasDeluca Surface Electromyography Detection&RecordingJuan Rodriguez IIIAún no hay calificaciones
- Depuracion de Mucus en Las Vias AereasDocumento7 páginasDepuracion de Mucus en Las Vias AereasFabian Esteban SubiabreAún no hay calificaciones
- Prevention of Endotracheal Suctioning-Induced Alveolar Derecruitment in Acute Lung InjuryDocumento54 páginasPrevention of Endotracheal Suctioning-Induced Alveolar Derecruitment in Acute Lung InjuryFabian Esteban SubiabreAún no hay calificaciones
- Citacion Vancouver PapersDocumento1 páginaCitacion Vancouver PapersFabian Esteban SubiabreAún no hay calificaciones
- Ventlacionmecanica ASMADocumento10 páginasVentlacionmecanica ASMAFabian Esteban SubiabreAún no hay calificaciones
- Patient Ventilator Asynchronies May TheDocumento8 páginasPatient Ventilator Asynchronies May TheFabian Esteban SubiabreAún no hay calificaciones
- 2015 Early Mobilization in The Critical Care Unit, A Review of Adult and Pediatric LiteratureDocumento9 páginas2015 Early Mobilization in The Critical Care Unit, A Review of Adult and Pediatric LiteratureFabian Esteban SubiabreAún no hay calificaciones
- Update en EpocDocumento9 páginasUpdate en EpocFabian Esteban SubiabreAún no hay calificaciones
- Physiology of Mechanical VentilationDocumento18 páginasPhysiology of Mechanical VentilationLiliana Andrea Hurtado MeraAún no hay calificaciones
- Extubation Failure Magnitude of The ProblemDocumento8 páginasExtubation Failure Magnitude of The ProblemFabian Esteban SubiabreAún no hay calificaciones
- The Effects of Orthostatism in Adult Intensive Care Unit PatientsDocumento8 páginasThe Effects of Orthostatism in Adult Intensive Care Unit PatientsFabian Esteban SubiabreAún no hay calificaciones
- A Chart of Failure Risk For NoninvasiveDocumento8 páginasA Chart of Failure Risk For NoninvasiveFabian Esteban SubiabreAún no hay calificaciones
- 116 093 Agustiag Oxygen Therapy During Exacerbations CopdDocumento6 páginas116 093 Agustiag Oxygen Therapy During Exacerbations CopdFabian Esteban SubiabreAún no hay calificaciones
- Endotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)Documento7 páginasEndotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)DCaeiroAún no hay calificaciones
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (120)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2101)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Initial Diagnosis and Management of ComaDocumento17 páginasInitial Diagnosis and Management of Comaguugle gogleAún no hay calificaciones
- Nursing Board Exam Review Questions in Emergency NursingDocumento17 páginasNursing Board Exam Review Questions in Emergency NursingAlsalman AnamAún no hay calificaciones
- Understanding Neurology - A Problem-Orientated Approach PDFDocumento241 páginasUnderstanding Neurology - A Problem-Orientated Approach PDFrys239Aún no hay calificaciones
- FOUR Score Instruction Guide For Application On MISH ICUDocumento2 páginasFOUR Score Instruction Guide For Application On MISH ICUMohamed Farouk El-FaresyAún no hay calificaciones
- Neurology PDFDocumento60 páginasNeurology PDFCahaya Al-HazeenillahAún no hay calificaciones
- Susruthasamhitha Part 1 PDFDocumento22 páginasSusruthasamhitha Part 1 PDFDr Suvarna NalapatAún no hay calificaciones
- M.M. College of Nursing, Mullana, Ambala: Medical Surgical Nursing Demonstration ON Neurological ExaminationDocumento12 páginasM.M. College of Nursing, Mullana, Ambala: Medical Surgical Nursing Demonstration ON Neurological ExaminationShitaljit IromAún no hay calificaciones
- Neurological ExaminationDocumento5 páginasNeurological Examinationshubham rathodAún no hay calificaciones
- GlasGow Coma ScaleDocumento3 páginasGlasGow Coma ScaleNathanielle Dae AquinoAún no hay calificaciones
- Approach To Emergency PatientDocumento18 páginasApproach To Emergency PatientJuan Pablo Gallardo ContrerasAún no hay calificaciones
- NMC CBT Mock Test 2Documento13 páginasNMC CBT Mock Test 2Charles Osiako100% (1)
- Self-Learning Module Unit 3 Physical AssessmentDocumento57 páginasSelf-Learning Module Unit 3 Physical AssessmentMarlon Glorioso IIAún no hay calificaciones
- UnconsciousnessDocumento16 páginasUnconsciousnessAkhilesh BabuAún no hay calificaciones
- Acute Stroke Nursing GuidelineFINAL 1 2Documento5 páginasAcute Stroke Nursing GuidelineFINAL 1 2radanikmaAún no hay calificaciones
- Pediatrics DDDocumento278 páginasPediatrics DDAyat AnnourAún no hay calificaciones
- NEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistDocumento12 páginasNEURO VITAL SIGNS ASSESSMENT Procedure and ChecklistMemer-alasadAún no hay calificaciones
- Osce Bank PDFDocumento15 páginasOsce Bank PDFnassir197083% (6)
- Neurology, Neurosurgery MCQ PointsDocumento32 páginasNeurology, Neurosurgery MCQ PointsBruno86% (7)
- Virginia PCRDocumento3 páginasVirginia PCRdandude505Aún no hay calificaciones
- Injury Severity ScoresDocumento32 páginasInjury Severity ScoresscribdnillyAún no hay calificaciones
- Neuro Assessment: The Single Most Important AssessmentDocumento10 páginasNeuro Assessment: The Single Most Important AssessmentpapadaadAún no hay calificaciones
- Mse OsceDocumento4 páginasMse OscejoryadelmAún no hay calificaciones
- Nursing NotesDocumento6 páginasNursing NotesAngel CauilanAún no hay calificaciones
- Brain Death - Malaysian Medical CouncilDocumento20 páginasBrain Death - Malaysian Medical CouncilAzizan Hakim0% (1)
- Assessment of The Trauma Patient PDFDocumento25 páginasAssessment of The Trauma Patient PDFcotovairinax100% (1)
- Reviewer For The Board Exam Part 1Documento34 páginasReviewer For The Board Exam Part 1jamchan100% (7)
- Level of ConsciousnessDocumento10 páginasLevel of ConsciousnessDinda Ramos100% (1)
- 15 Item ACLS Drill Answers and RationaleDocumento6 páginas15 Item ACLS Drill Answers and RationaleAijem RyanAún no hay calificaciones
- Assessing ConsciousnessDocumento25 páginasAssessing ConsciousnessDrGasnas100% (1)
- ABC TraumaDocumento27 páginasABC TraumarikarzAún no hay calificaciones