También podría gustarte
- 1.emollients Prescribing Guideline Sept 2013Documento4 páginas1.emollients Prescribing Guideline Sept 2013kyle31Aún no hay calificaciones
- Taking A Dermatological History - Dermatology - FastbleepDocumento5 páginasTaking A Dermatological History - Dermatology - Fastbleepkyle31Aún no hay calificaciones
- Necessary Elements of A Dermatologic History and Physical Evaluation PDFDocumento9 páginasNecessary Elements of A Dermatologic History and Physical Evaluation PDFkyle31Aún no hay calificaciones
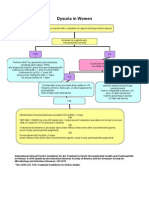
- Women With Dysuria AlgorhtmDocumento1 páginaWomen With Dysuria Algorhtmkyle31Aún no hay calificaciones
- AntihypertensiveDocumento1 páginaAntihypertensivekyle31Aún no hay calificaciones
- A Brief Review: The Epidemiology of Acquired Melanocytic NeviDocumento9 páginasA Brief Review: The Epidemiology of Acquired Melanocytic Nevikyle31Aún no hay calificaciones
- Marsupialization of A Bartholin's Cyst or AbscessDocumento2 páginasMarsupialization of A Bartholin's Cyst or Abscesskyle31Aún no hay calificaciones
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- A Collaborative Retrospective Study On The Efficacy and Safety of Intravitreal Dexamethasone Implant (Ozurdex) in Patients With Diabetic Macular EdemaDocumento17 páginasA Collaborative Retrospective Study On The Efficacy and Safety of Intravitreal Dexamethasone Implant (Ozurdex) in Patients With Diabetic Macular EdemaJosé Díaz OficialAún no hay calificaciones
- Aging With Grace What The Nun Study Teaches Us AboDocumento6 páginasAging With Grace What The Nun Study Teaches Us Aboandrea chinchillaAún no hay calificaciones
- Lucid Dreaming - Lucid Dreams - A Beginner's Guide On How To Control Your Dreams With Different Techniques PDFDocumento127 páginasLucid Dreaming - Lucid Dreams - A Beginner's Guide On How To Control Your Dreams With Different Techniques PDFMargarita Petrova50% (2)
- Chapter 1 - Introduction and HistoryDocumento37 páginasChapter 1 - Introduction and HistoryTwinkle ParmarAún no hay calificaciones
- 2013-14 Rotary Annual Report PDFDocumento32 páginas2013-14 Rotary Annual Report PDFAmri KosmarAún no hay calificaciones
- 659 1764 1 PBDocumento11 páginas659 1764 1 PBAgita GusmiarnyAún no hay calificaciones
- What Is Child PsychologyDocumento16 páginasWhat Is Child PsychologyTalha MughalAún no hay calificaciones
- Cefuroxime (Drug Study)Documento2 páginasCefuroxime (Drug Study)Rosebel LaguraAún no hay calificaciones
- Anesthetics: Local Topical: Name Indications Peak Effect (Min) Duration (Min) AmidesDocumento3 páginasAnesthetics: Local Topical: Name Indications Peak Effect (Min) Duration (Min) Amidesammar amerAún no hay calificaciones
- Group 1 - Posterior Disk Bulge at L5-S1 With Bilateral Severe Neural Canal Narrowing PDFDocumento7 páginasGroup 1 - Posterior Disk Bulge at L5-S1 With Bilateral Severe Neural Canal Narrowing PDFKatAún no hay calificaciones
- Patient Education Pneumonia 1.1Documento3 páginasPatient Education Pneumonia 1.1Cuttie Anne GalangAún no hay calificaciones
- AffiliationsDocumento9 páginasAffiliationsGurpreet CharaAún no hay calificaciones
- Definition of Terms: Herbaceous Plant Costaceae Brazil Bahia Espirito SantoDocumento1 páginaDefinition of Terms: Herbaceous Plant Costaceae Brazil Bahia Espirito SantoAshly Jamiah DelRosario ManatoAún no hay calificaciones
- Ambulatory Blood Pressure Monitoring in Children and Adolescents: 2022 Update: A Scientific Statement From The American Heart AssociationDocumento11 páginasAmbulatory Blood Pressure Monitoring in Children and Adolescents: 2022 Update: A Scientific Statement From The American Heart AssociationWaleed saleemAún no hay calificaciones
- Health Checklist Health Checklist: Temperature: Time Taken: Temperature: Time TakenDocumento1 páginaHealth Checklist Health Checklist: Temperature: Time Taken: Temperature: Time TakenHelen Paragas Solivar AranetaAún no hay calificaciones
- MS CourseTask8Documento3 páginasMS CourseTask8Aria100% (1)
- GEHC Invenia ABUS Breast Density InfoDocumento2 páginasGEHC Invenia ABUS Breast Density InfoCarmen Suárez GarcíaAún no hay calificaciones
- ISO STANDARD METHODS FOR MICROBIOLOGICAL TESTING (L. Monocytogenes)Documento11 páginasISO STANDARD METHODS FOR MICROBIOLOGICAL TESTING (L. Monocytogenes)Abhimanyu BagalAún no hay calificaciones
- Health Assessment ON Gastro Intestinal System: Submitted To: Submitted byDocumento13 páginasHealth Assessment ON Gastro Intestinal System: Submitted To: Submitted byAnanthibalaAún no hay calificaciones
- Management of Renal Stones: Theme From January 2013 ExamDocumento123 páginasManagement of Renal Stones: Theme From January 2013 ExamBela VitoriaAún no hay calificaciones
- Pediatric Nursing Care (Case Study)Documento37 páginasPediatric Nursing Care (Case Study)mira utami ningsih80% (46)
- Inform Consent HIVDocumento465 páginasInform Consent HIVHartini100% (2)
- NCM 104 Musculo Skeletal QuizDocumento280 páginasNCM 104 Musculo Skeletal Quizmarvinmadrid2003Aún no hay calificaciones
- "Insanity As A Defence Under Sec.84 of IPC": Academic SessionDocumento14 páginas"Insanity As A Defence Under Sec.84 of IPC": Academic SessionAbhishekAún no hay calificaciones
- Ectopic Pregnancy: Deomicah D. SolanoDocumento42 páginasEctopic Pregnancy: Deomicah D. SolanoJann ericka JaoAún no hay calificaciones
- 1678816971346634Documento47 páginas1678816971346634SophiyaAún no hay calificaciones
- Role-Taking 223143219 Lenient Anele NkalaDocumento8 páginasRole-Taking 223143219 Lenient Anele NkalaAnele NkalaAún no hay calificaciones
- IHD - JalalDocumento46 páginasIHD - JalalMituran IshwarAún no hay calificaciones
- Blood Groups, Blood Transfusion & Rhesus FactorDocumento38 páginasBlood Groups, Blood Transfusion & Rhesus FactorUzma KhanAún no hay calificaciones
- Jyotish - 1980 - Saha - Precious Stones That Heal PDFDocumento258 páginasJyotish - 1980 - Saha - Precious Stones That Heal PDFKrishan Sirohiya100% (1)