También podría gustarte
- One Way ANOVADocumento2 páginasOne Way ANOVAharyroyAún no hay calificaciones
- Proven Clinical Efficacy Makes Liverubin the Ultimate Liver ShieldDocumento28 páginasProven Clinical Efficacy Makes Liverubin the Ultimate Liver ShieldharyroyAún no hay calificaciones
- Market Share of Hair Care Brands in India From 2017 To 2019Documento8 páginasMarket Share of Hair Care Brands in India From 2017 To 2019haryroyAún no hay calificaciones
- Beauty-Personal-Care Personal-Care Hair-Care India INR enDocumento12 páginasBeauty-Personal-Care Personal-Care Hair-Care India INR enharyroyAún no hay calificaciones
- Statista Consumer Market Outlook for Beauty & Personal Care in IndiaDocumento13 páginasStatista Consumer Market Outlook for Beauty & Personal Care in IndiaharyroyAún no hay calificaciones
- NtbtlogDocumento36 páginasNtbtlogharyroyAún no hay calificaciones
- Beauty-Personal-Care Personal-Care Hair-Care India INR enDocumento12 páginasBeauty-Personal-Care Personal-Care Hair-Care India INR enharyroyAún no hay calificaciones
- Presentation1 For Investors MainDocumento4 páginasPresentation1 For Investors MainharyroyAún no hay calificaciones
- REGRESSION DATADocumento8 páginasREGRESSION DATAharyroyAún no hay calificaciones
- India's $14B beauty industryDocumento71 páginasIndia's $14B beauty industryharyroyAún no hay calificaciones
- Market Share of Hair Care Brands in India From 2017 To 2019Documento8 páginasMarket Share of Hair Care Brands in India From 2017 To 2019haryroyAún no hay calificaciones
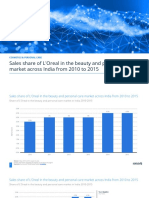
- Statistic - Id670452 - Share of Loreal in The Beauty and Personal Care Market in India 2010 2015Documento8 páginasStatistic - Id670452 - Share of Loreal in The Beauty and Personal Care Market in India 2010 2015haryroyAún no hay calificaciones
- Refund TxtcdsDocumento1 páginaRefund TxtcdsharyroyAún no hay calificaciones
- BdlogDocumento2 páginasBdlogRizka Pradini RionitaAún no hay calificaciones
- Password AGREDocumento1 páginaPassword AGREharyroyAún no hay calificaciones
- Password Query - txtARGADocumento1 páginaPassword Query - txtARGAharyroyAún no hay calificaciones
- Out of StockADRGAEGDocumento1 páginaOut of StockADRGAEGharyroyAún no hay calificaciones
- Payment EWFEWDocumento1 páginaPayment EWFEWharyroyAún no hay calificaciones
- Order Return StateASSGRFADocumento1 páginaOrder Return StateASSGRFAharyroyAún no hay calificaciones
- Order Customer CommentZXVCDocumento1 páginaOrder Customer CommentZXVCharyroyAún no hay calificaciones
- Log alertAERGWEGEDocumento1 páginaLog alertAERGWEGEharyroyAún no hay calificaciones
- Order Customer CommentZXVCDocumento1 páginaOrder Customer CommentZXVCharyroyAún no hay calificaciones
- Employee PasswordDocumento1 páginaEmployee PasswordharyroyAún no hay calificaciones
- Order CanceledDFVADFVDocumento1 páginaOrder CanceledDFVADFVharyroyAún no hay calificaciones
- Guest To CustomerEWFDdfDocumento1 páginaGuest To CustomerEWFDdfharyroyAún no hay calificaciones
- Backoffice OrderresDocumento1 páginaBackoffice OrderresharyroyAún no hay calificaciones
- Newsletter EWFRWFDocumento1 páginaNewsletter EWFRWFharyroyAún no hay calificaciones
- Credit SliprfWFSdDocumento1 páginaCredit SliprfWFSdharyroyAún no hay calificaciones
- Contact REFVSQADocumento1 páginaContact REFVSQAharyroyAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Infrared Spectroscopy in Medical Diagnostics - Advances in Instrumentation For Glycemic Control and ApplicationsDocumento4 páginasInfrared Spectroscopy in Medical Diagnostics - Advances in Instrumentation For Glycemic Control and ApplicationsJuan MartínezAún no hay calificaciones
- Topical Generic Bioequivalence Assessment MethodsDocumento38 páginasTopical Generic Bioequivalence Assessment MethodsDiana LeonAún no hay calificaciones
- Continuous Glucose Profiles in Healthy Subjects Under Everyday Life Conditions and After Different MealsDocumento9 páginasContinuous Glucose Profiles in Healthy Subjects Under Everyday Life Conditions and After Different MealsAsose TuAún no hay calificaciones
- Hasler1997 OkDocumento10 páginasHasler1997 OkRamiro Manzano NúñezAún no hay calificaciones
- Nasim Rezvanis CVDocumento3 páginasNasim Rezvanis CVapi-548808668Aún no hay calificaciones
- Eicom As 700 BrochureDocumento3 páginasEicom As 700 Brochurer_routhierAún no hay calificaciones
- Neurotransmission, Measuring Chemical Events In: Advanced ArticleDocumento12 páginasNeurotransmission, Measuring Chemical Events In: Advanced ArticleazzaassAún no hay calificaciones
- Mode of Action of Cupping Local Metabolism and Pain Thresholds in Neck Pain Patients and Healthy Subjects 2014Documento11 páginasMode of Action of Cupping Local Metabolism and Pain Thresholds in Neck Pain Patients and Healthy Subjects 2014silkofosAún no hay calificaciones
- Zhanfeng Cui PDFDocumento22 páginasZhanfeng Cui PDFsdfdsfAún no hay calificaciones
- Non-Invasive Glucose SensorsDocumento12 páginasNon-Invasive Glucose SensorsGerman GodiAún no hay calificaciones
- MEMBRANE TECHNIQUES Dialysis and Reverse OsmosisDocumento10 páginasMEMBRANE TECHNIQUES Dialysis and Reverse OsmosisAlexis Jara VidalAún no hay calificaciones
- In-Process Control of Insulin Production by High-Performance Liquid ChromatographyDocumento7 páginasIn-Process Control of Insulin Production by High-Performance Liquid ChromatographyicedjesuschristAún no hay calificaciones
- 2018 CONTINUUM Multimodality Monitoring in The Neurocritical Care UnitDocumento13 páginas2018 CONTINUUM Multimodality Monitoring in The Neurocritical Care UnitKarl Jimenez SeparaAún no hay calificaciones
- Oliver Et Al., 2009 Glucose Sensors-A ReviewDocumento14 páginasOliver Et Al., 2009 Glucose Sensors-A ReviewMoisi XhoxhiAún no hay calificaciones
- MEM Devices For Drug DeliveryDocumento52 páginasMEM Devices For Drug DeliveryTechnautsAún no hay calificaciones
- Adv Materials Inter - 2023 - Saifullah - Sampling Dermal Interstitial Fluid Using Microneedles A Review of RecentDocumento23 páginasAdv Materials Inter - 2023 - Saifullah - Sampling Dermal Interstitial Fluid Using Microneedles A Review of RecentAndisheh ChoupaniAún no hay calificaciones
- 40 Years of Microdialysis 2014 BerlinDocumento30 páginas40 Years of Microdialysis 2014 BerlinUrban UngerstedtAún no hay calificaciones