También podría gustarte
- 5 Revathi EtalDocumento5 páginas5 Revathi EtaleditorijmrhsAún no hay calificaciones
- Correlation of Dyslipidemia and Type 2 Diabetes Mellitus Amongst The People of Vidarbha Region of IndiaDocumento6 páginasCorrelation of Dyslipidemia and Type 2 Diabetes Mellitus Amongst The People of Vidarbha Region of IndiaKiki FatmawatyAún no hay calificaciones
- Enmet DMDocumento7 páginasEnmet DMAreef MuarifAún no hay calificaciones
- Research ArticleDocumento7 páginasResearch ArticleRicardo Joshua RojasAún no hay calificaciones
- Tovar Et Al-2017-Molecular Nutrition & Food ResearchDocumento12 páginasTovar Et Al-2017-Molecular Nutrition & Food ResearchRal T. BerensAún no hay calificaciones
- Plasma MDA and Erythrocyte Catalase in DiabetesDocumento14 páginasPlasma MDA and Erythrocyte Catalase in DiabetesKyae Mhon HtweAún no hay calificaciones
- Antioxidant Effects of Zinc Supplementation in Tunisians With Type 2 Diabetes MellitusDocumento6 páginasAntioxidant Effects of Zinc Supplementation in Tunisians With Type 2 Diabetes MellitusgautomsahariaAún no hay calificaciones
- Supersize Teens - The Metabolic Syndrome.Documento23 páginasSupersize Teens - The Metabolic Syndrome.Milon MitraAún no hay calificaciones
- Beneficial Effects of Viscous Dietary Fiber From Konjac-Mannan in Subjects With The Insulin Resistance Syndro M eDocumento6 páginasBeneficial Effects of Viscous Dietary Fiber From Konjac-Mannan in Subjects With The Insulin Resistance Syndro M eNaresh MaliAún no hay calificaciones
- Article - Ghrelin and Leptin in Insulin Resistance (CHECKED)Documento6 páginasArticle - Ghrelin and Leptin in Insulin Resistance (CHECKED)pixoguiasAún no hay calificaciones
- Alasan Ke ManusiaDocumento12 páginasAlasan Ke ManusiaafiwahyuAún no hay calificaciones
- Study links dyslipidemia to type 2 diabetesDocumento5 páginasStudy links dyslipidemia to type 2 diabetesDinesshia pwsAún no hay calificaciones
- Jurnal PH 13Documento9 páginasJurnal PH 13ruthameliapAún no hay calificaciones
- Final Draft - Surya Bagaskara - Identifying Risk Factors of Prediabetes in Prehypertension PopulationDocumento10 páginasFinal Draft - Surya Bagaskara - Identifying Risk Factors of Prediabetes in Prehypertension PopulationHerfandi DimasAún no hay calificaciones
- L Carnosine in DiabetesDocumento11 páginasL Carnosine in DiabetesVivekAún no hay calificaciones
- CRP, Lipids, BMI Higher in Sudanese T2DM PatientsDocumento9 páginasCRP, Lipids, BMI Higher in Sudanese T2DM PatientsMotasem Sirag Mohmmed othmanAún no hay calificaciones
- AnnotationsDocumento3 páginasAnnotationsAegina FestinAún no hay calificaciones
- HbA1C AS AN INDEX OF GLYCEMIC STATUS IN OBESE TYPE 2 DIABETICSDocumento6 páginasHbA1C AS AN INDEX OF GLYCEMIC STATUS IN OBESE TYPE 2 DIABETICSInternational Journal of Clinical and Biomedical Research (IJCBR)Aún no hay calificaciones
- Paper DM NutritionDocumento10 páginasPaper DM NutritionyinvilllAún no hay calificaciones
- Nonalcoholic SteatohepatitisDocumento15 páginasNonalcoholic SteatohepatitisLucas VenturaAún no hay calificaciones
- Dietary Pattern of Nopal, Chia Seed, Soy and Oats Reduces Metabolic Syndrome Risk FactorsDocumento6 páginasDietary Pattern of Nopal, Chia Seed, Soy and Oats Reduces Metabolic Syndrome Risk FactorsMontserrat JiménezAún no hay calificaciones
- Study of Lipid Peroxide and Lipid Profile in Diabetes MellitusDocumento5 páginasStudy of Lipid Peroxide and Lipid Profile in Diabetes Mellitusewo jatmikoAún no hay calificaciones
- 7decaf9c Cb18 4623 Bced Ecef2197e451Documento25 páginas7decaf9c Cb18 4623 Bced Ecef2197e451PrabhuAún no hay calificaciones
- Relationship Between Serum Ferritin Level and Hba in Bangladeshi Type 2 Diabetic PatientsDocumento5 páginasRelationship Between Serum Ferritin Level and Hba in Bangladeshi Type 2 Diabetic PatientsdebbykgAún no hay calificaciones
- Low-density lipoprotein cholesterol as predictor of metabolic syndrome riskDocumento7 páginasLow-density lipoprotein cholesterol as predictor of metabolic syndrome riskAndi SuryawanAún no hay calificaciones
- Impact of lifestyle changes on obese childrenDocumento5 páginasImpact of lifestyle changes on obese childrensebastianAún no hay calificaciones
- IOSR Journal of Pharmacy (IOSRPHR)Documento6 páginasIOSR Journal of Pharmacy (IOSRPHR)IOSR Journal of PharmacyAún no hay calificaciones
- Bantuan Hidup Dasar SDKDocumento22 páginasBantuan Hidup Dasar SDKghea_86Aún no hay calificaciones
- Risk Factors For Coronary Heart Disease in Type Ii Diabetes MellitusDocumento6 páginasRisk Factors For Coronary Heart Disease in Type Ii Diabetes MellitusmahalAún no hay calificaciones
- Alhamdulillah Ada JurnalnyaDocumento6 páginasAlhamdulillah Ada JurnalnyaNovriman LiviaAún no hay calificaciones
- The Relationship Between Hba1C and Lipid Profile in Type 2 Diabetic Saudi PatientsDocumento6 páginasThe Relationship Between Hba1C and Lipid Profile in Type 2 Diabetic Saudi PatientsnaxxxAún no hay calificaciones
- Euu 2Documento10 páginasEuu 2Johanna GalvisAún no hay calificaciones
- Micronutrientes en DiabetesDocumento6 páginasMicronutrientes en Diabetesluis Gomez VallejoAún no hay calificaciones
- 05 Iajps05062017Documento6 páginas05 Iajps05062017Baru Chandrasekhar RaoAún no hay calificaciones
- Relation of A Variant in Adiponectin Gene (rs266729) With Metabolic Syndrome and Diabetes Mellitus Type 2 in Adult Obese SubjectsDocumento7 páginasRelation of A Variant in Adiponectin Gene (rs266729) With Metabolic Syndrome and Diabetes Mellitus Type 2 in Adult Obese SubjectsVivi yenni aryantiAún no hay calificaciones
- Amj 05 429 PDFDocumento7 páginasAmj 05 429 PDFBachtiar M TaUfikAún no hay calificaciones
- Double Trouble: MAFLD and Diabetes CoexistenceDocumento16 páginasDouble Trouble: MAFLD and Diabetes CoexistenceFarjana NajninAún no hay calificaciones
- Kefir Improves Blood Parameters and Reduces Cardiovascular Risks in Patients With Metabolic SyndromeDocumento7 páginasKefir Improves Blood Parameters and Reduces Cardiovascular Risks in Patients With Metabolic SyndromeCristina OliveiraAún no hay calificaciones
- 7 FFCDocumento8 páginas7 FFCHow to youAún no hay calificaciones
- Antocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Documento9 páginasAntocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Elenice Peltz NutricionistaAún no hay calificaciones
- Order - 523187 - Main Document With Abstract - TRACKED - REVISEDDocumento12 páginasOrder - 523187 - Main Document With Abstract - TRACKED - REVISEDAn MAún no hay calificaciones
- Articulo Dislipidemias 2Documento18 páginasArticulo Dislipidemias 2DANIELA CALDERON SAGAHONAún no hay calificaciones
- L Argina PDFDocumento6 páginasL Argina PDFAnyi VargasAún no hay calificaciones
- Obesity and Type 2 Diabetes ThesisDocumento6 páginasObesity and Type 2 Diabetes Thesisafhbexrci100% (1)
- Gudoy, Charies Jamille 12-WeierstrassDocumento4 páginasGudoy, Charies Jamille 12-WeierstrasschaAún no hay calificaciones
- A CORRELATIVE STUDY OF RED MEAT CONSUMPTION AND CARDIO METABOLIC RISK FACTORS IN YOUNG AND AGED FEMALE PATIENTS OF TYPE 2 DIABETES DR - Satish Kumar NS1, MD, Mrs - Pavana K2, DR - Aswini Dutt R3, MDDocumento6 páginasA CORRELATIVE STUDY OF RED MEAT CONSUMPTION AND CARDIO METABOLIC RISK FACTORS IN YOUNG AND AGED FEMALE PATIENTS OF TYPE 2 DIABETES DR - Satish Kumar NS1, MD, Mrs - Pavana K2, DR - Aswini Dutt R3, MDiajpsAún no hay calificaciones
- Al Shehri 2008Documento10 páginasAl Shehri 2008Dewi MaryamAún no hay calificaciones
- 6340 25219 1 PB PDFDocumento3 páginas6340 25219 1 PB PDFChris Jo ManojAún no hay calificaciones
- Dietary Knowledge Among Adults With Type 2 Diabetes-Kingdom of Saudi ArabiaDocumento8 páginasDietary Knowledge Among Adults With Type 2 Diabetes-Kingdom of Saudi ArabiaMahmoud HakimAún no hay calificaciones
- Sindroma MetabolikDocumento7 páginasSindroma MetabolikainindyaAún no hay calificaciones
- Significance of Orlistat for Dyslipidemia, SBP, and BMIDocumento7 páginasSignificance of Orlistat for Dyslipidemia, SBP, and BMIGestne AureAún no hay calificaciones
- Cinnamon Low Blood GlucoseDocumento4 páginasCinnamon Low Blood GlucoseMayene ChavezAún no hay calificaciones
- Nutrients 13 00865Documento11 páginasNutrients 13 00865Roger CAún no hay calificaciones
- Adiponectin Levels in Children with Type 1 DiabetesDocumento2 páginasAdiponectin Levels in Children with Type 1 DiabetespratamamdAún no hay calificaciones
- Jurnal Gita 6Documento7 páginasJurnal Gita 6dedeandikaAún no hay calificaciones
- Jurnal DR AyukDocumento6 páginasJurnal DR Ayukmerina selviraAún no hay calificaciones
- Metabolic Syndrome as a Predictor of DiabetesDocumento10 páginasMetabolic Syndrome as a Predictor of DiabetesChiranjeeviAún no hay calificaciones
- AyunoDocumento8 páginasAyunoRaul DavilaAún no hay calificaciones
- Are The Associations of Plasma Leptin and Adiponectin With Type 2 Diabetes Independent of Obesity in Older Chinese Adults?Documento6 páginasAre The Associations of Plasma Leptin and Adiponectin With Type 2 Diabetes Independent of Obesity in Older Chinese Adults?bogdansoroAún no hay calificaciones
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryDe EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryCalificación: 5 de 5 estrellas5/5 (1)
- 129 PDFDocumento10 páginas129 PDFewo jatmikoAún no hay calificaciones
- Triage Education KitDocumento75 páginasTriage Education KitJimmyAún no hay calificaciones
- Us Diagnosis of Breast CancerDocumento14 páginasUs Diagnosis of Breast Cancerewo jatmikoAún no hay calificaciones
- Original Article Paederus Dermatitis in South IndiaDocumento6 páginasOriginal Article Paederus Dermatitis in South Indiasoumalya481Aún no hay calificaciones
- MCQs For MRCOG Part 1 A Self-Assessment Guide PDF BookDocumento118 páginasMCQs For MRCOG Part 1 A Self-Assessment Guide PDF BookAhmed Abdelmonsef Albashatly86% (14)
- Networking and ComputerDocumento18 páginasNetworking and Computerewo jatmikoAún no hay calificaciones
- Study of Lipid Peroxide and Lipid Profile in Diabetes MellitusDocumento5 páginasStudy of Lipid Peroxide and Lipid Profile in Diabetes Mellitusewo jatmikoAún no hay calificaciones
- JAnaesthClinPharmacol29166-2035828 053918Documento5 páginasJAnaesthClinPharmacol29166-2035828 053918ewo jatmikoAún no hay calificaciones
- Usg DetectionDocumento7 páginasUsg Detectionewo jatmikoAún no hay calificaciones
- Epidemiology of TuberculosisDocumento21 páginasEpidemiology of TuberculosisAmrina RosyadaAún no hay calificaciones
- Beta Met Has One Rcog GuidelineDocumento9 páginasBeta Met Has One Rcog GuidelineShefali MahindruAún no hay calificaciones
- Antioxydant - Preeclampsia PDFDocumento88 páginasAntioxydant - Preeclampsia PDFewo jatmikoAún no hay calificaciones
- Open Fracture (Edit)Documento9 páginasOpen Fracture (Edit)rantiningsihsumarniAún no hay calificaciones
- Pi Is 0020729296027518Documento2 páginasPi Is 0020729296027518ewo jatmikoAún no hay calificaciones
- Medical Professionalism Blok 1 '10Documento22 páginasMedical Professionalism Blok 1 '10ewo jatmikoAún no hay calificaciones
- Antenatal Care: Routine Care For The Healthy Pregnant WomanDocumento304 páginasAntenatal Care: Routine Care For The Healthy Pregnant WomanNadia Gina AnggrainiAún no hay calificaciones
- Routine Antenatal Care For Healthy Pregnant WomenDocumento44 páginasRoutine Antenatal Care For Healthy Pregnant Womenewo jatmikoAún no hay calificaciones
- Preface: Best Practice & Research Clinical Endocrinology & Metabolism Vol. 21, No. 2, Pp. Vii-Viii, 2007Documento2 páginasPreface: Best Practice & Research Clinical Endocrinology & Metabolism Vol. 21, No. 2, Pp. Vii-Viii, 2007ewo jatmikoAún no hay calificaciones
- Polys Ovary Syndrome No33Documento8 páginasPolys Ovary Syndrome No33ewo jatmikoAún no hay calificaciones
- Brain Attack Definition An Did of Stroke Present A It OnDocumento36 páginasBrain Attack Definition An Did of Stroke Present A It OnchirahmawatiAún no hay calificaciones
- Management OA Kuliah 2aw97Documento108 páginasManagement OA Kuliah 2aw97ewo jatmikoAún no hay calificaciones
- Routine Antenatal Care For Healthy Pregnant WomenDocumento44 páginasRoutine Antenatal Care For Healthy Pregnant Womenewo jatmikoAún no hay calificaciones
- PBL FILOSOFI DAN KEBERMANFAATANNYADocumento27 páginasPBL FILOSOFI DAN KEBERMANFAATANNYALetchumana KrishnanAún no hay calificaciones
- Obat Analgesik Ains 2009-15Documento34 páginasObat Analgesik Ains 2009-15ewo jatmikoAún no hay calificaciones
- Obat Analgesik Ains 2009-15Documento34 páginasObat Analgesik Ains 2009-15ewo jatmikoAún no hay calificaciones
- Management OA Kuliah 2aw97Documento108 páginasManagement OA Kuliah 2aw97ewo jatmikoAún no hay calificaciones
- TUTORIAL OkDocumento37 páginasTUTORIAL Okewo jatmikoAún no hay calificaciones
- Concentration/Mem Ory: by Sri Sundari PurbohadiDocumento23 páginasConcentration/Mem Ory: by Sri Sundari PurbohadiResdanggaHusadaAún no hay calificaciones
- Jurnal AppendicitisDocumento10 páginasJurnal AppendicitisEwoJatmikoAún no hay calificaciones
- M.Owais - 18EL46 (Assignment 2)Documento6 páginasM.Owais - 18EL46 (Assignment 2)Islam CandleAún no hay calificaciones
- Philippines Province Boosts Local Health SystemDocumento12 páginasPhilippines Province Boosts Local Health Systemebc07Aún no hay calificaciones
- Tackling Obesity in The Western WorldDocumento7 páginasTackling Obesity in The Western WorldLê Hoàng HiệpAún no hay calificaciones
- Carrer Objective: Curriculam VitaeDocumento4 páginasCarrer Objective: Curriculam VitaeJAYRAM PATILAún no hay calificaciones
- Keto A Womans Guide - Tasha Metcalf PDFDocumento245 páginasKeto A Womans Guide - Tasha Metcalf PDFMakenzie MurrayAún no hay calificaciones
- Gizi - Obesitas - KLP VDocumento23 páginasGizi - Obesitas - KLP VAD 21Aún no hay calificaciones
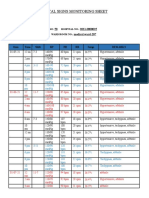
- Vital Signs Monitoring SheetDocumento2 páginasVital Signs Monitoring SheetRenea Joy ArruejoAún no hay calificaciones
- Prevalence of Underweight Stunting and Thinness AmDocumento8 páginasPrevalence of Underweight Stunting and Thinness AmCar OrdzAún no hay calificaciones
- IAP GuidebookDocumento21 páginasIAP Guidebooksuheena.CAún no hay calificaciones
- Life 11 00532Documento15 páginasLife 11 00532grpadillaAún no hay calificaciones
- PE BMI Lesson SimulationDocumento12 páginasPE BMI Lesson SimulationGerald TeañoAún no hay calificaciones
- Daftar Pustaka: Strokenews/Coronary-Arterydisease - The-Abcs Ofcad - Ucm - 436416 - Article - JSPDocumento3 páginasDaftar Pustaka: Strokenews/Coronary-Arterydisease - The-Abcs Ofcad - Ucm - 436416 - Article - JSPmuhamad isafarudinAún no hay calificaciones
- BMI W HFA Validated (3!24!2017)Documento151 páginasBMI W HFA Validated (3!24!2017)jeffordillasAún no hay calificaciones
- Too Much Sitting - A Health Hazard - ScienceDirectDocumento2 páginasToo Much Sitting - A Health Hazard - ScienceDirectAngelo PintalAún no hay calificaciones
- Chapter-7 Test Measurement and Evaluation Class-11Documento10 páginasChapter-7 Test Measurement and Evaluation Class-11Ashutosh DayalAún no hay calificaciones
- Across Sectionalstudyontheassociationbetweensocialmediaaddictionbodyimageandsocialcomparisonamongyoungadultfilipinowomenaged18 25yearsoldinMetroManilaDocumento11 páginasAcross Sectionalstudyontheassociationbetweensocialmediaaddictionbodyimageandsocialcomparisonamongyoungadultfilipinowomenaged18 25yearsoldinMetroManilaNhiel jaztine LlanderalAún no hay calificaciones
- Essay 16 - 2Documento1 páginaEssay 16 - 2Sofya SorokinaAún no hay calificaciones
- Mpu 2312Documento15 páginasMpu 2312Sherly TanAún no hay calificaciones
- (1479683X - European Journal of Endocrinology) ENDOCRINE OBESITY - Pituitary Dysfunction in ObesityDocumento14 páginas(1479683X - European Journal of Endocrinology) ENDOCRINE OBESITY - Pituitary Dysfunction in ObesityAnonymous nRufcMpvNAún no hay calificaciones
- A Community Perspective of COVID 19 and Obesity in Children 2021 Obesity MedDocumento6 páginasA Community Perspective of COVID 19 and Obesity in Children 2021 Obesity MedpangaribuansantaAún no hay calificaciones
- Bagi Percakapan EnglishDocumento4 páginasBagi Percakapan EnglishFatimatuz ZahroAún no hay calificaciones
- Ielts Trainer 2 - Reading 2 - Correcting PapersDocumento5 páginasIelts Trainer 2 - Reading 2 - Correcting PapersSơn CápAún no hay calificaciones
- Grade 6 PPT Health q1 Lesson 1Documento29 páginasGrade 6 PPT Health q1 Lesson 1Jeffrey MirandaAún no hay calificaciones
- Lesson 3: Let's Be Health Aware!: Activity 1: Describe Me in My PictureDocumento5 páginasLesson 3: Let's Be Health Aware!: Activity 1: Describe Me in My PictureJon Tracy Azuelo100% (1)
- Importance of An Active LifestyleDocumento2 páginasImportance of An Active LifestyleDreamCatcher Insommia18Aún no hay calificaciones
- Body ShamingDocumento2 páginasBody ShamingJezeil Dimas100% (3)
- 2020 Ottawa Classic - Final Placings With OverallsDocumento7 páginas2020 Ottawa Classic - Final Placings With Overallsspam emailAún no hay calificaciones
- 2021 Anthropometry Procedures Manual 508Documento91 páginas2021 Anthropometry Procedures Manual 508Diogo JuniorAún no hay calificaciones
- Scoring in PFTDocumento3 páginasScoring in PFTNoel BandaAún no hay calificaciones
- Obesity - The Health Time Bomb: ©LTPHN 2008Documento36 páginasObesity - The Health Time Bomb: ©LTPHN 2008EVA PUTRANTO100% (2)