También podría gustarte
- The Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingDe EverandThe Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingJanindra WarusavitarneAún no hay calificaciones
- Los Terrybles Book TeamDocumento9 páginasLos Terrybles Book TeamWildor Herrera GuevaraAún no hay calificaciones
- Liver Transplantation For Biliary Atresia : Thomas E. Starz), M.D., Ph.D. Carlos O. Esquivel, M.D., PH.DDocumento8 páginasLiver Transplantation For Biliary Atresia : Thomas E. Starz), M.D., Ph.D. Carlos O. Esquivel, M.D., PH.DPratita Jati PermatasariAún no hay calificaciones
- Surgery For Duodenal Ulcer PDFDocumento10 páginasSurgery For Duodenal Ulcer PDFRuel P. AgustinAún no hay calificaciones
- Difficult Acute Cholecystitis: Treatment and Technical IssuesDe EverandDifficult Acute Cholecystitis: Treatment and Technical IssuesAún no hay calificaciones
- IleostomyDocumento7 páginasIleostomyPavan KumarAún no hay calificaciones
- Mainz II Surgery IllustratedDocumento25 páginasMainz II Surgery IllustratedPurvi ParikhAún no hay calificaciones
- Ileal Neobladder and Its Variants: Georgios Gakis, Arnulf StenzlDocumento9 páginasIleal Neobladder and Its Variants: Georgios Gakis, Arnulf StenzlRara Aulia IIAún no hay calificaciones
- Colecistogastrostomia-Biopsia de HigadoDocumento8 páginasColecistogastrostomia-Biopsia de HigadoWildor Herrera GuevaraAún no hay calificaciones
- Laparoscopic Cholecystectomy - StatPearls - NCBI BookshelfDocumento1 páginaLaparoscopic Cholecystectomy - StatPearls - NCBI BookshelfOmar HamwiAún no hay calificaciones
- Hepatico JDocumento4 páginasHepatico Jcharie2Aún no hay calificaciones
- Urinary DiversionDocumento44 páginasUrinary Diversionminnalesri100% (1)
- Small Nowel Emergency SurgeryDocumento8 páginasSmall Nowel Emergency SurgerySurya Nirmala DewiAún no hay calificaciones
- Pi Is 2213576614000049Documento3 páginasPi Is 2213576614000049Ditha FadhilaAún no hay calificaciones
- Remove Them Within A Week. Mainz Neobladder: Chapter 189: Supravesical Urinary DiversionDocumento1 páginaRemove Them Within A Week. Mainz Neobladder: Chapter 189: Supravesical Urinary DiversioncesaliapAún no hay calificaciones
- Basics of Intestinal Surgery: Anatomy, Pathophysiology, Instrumentation & SuturingDocumento8 páginasBasics of Intestinal Surgery: Anatomy, Pathophysiology, Instrumentation & SuturingakreditasirsurAún no hay calificaciones
- Urinary DiversionDocumento11 páginasUrinary Diversionvlad910Aún no hay calificaciones
- Argh - Ms.id.555581, DR Muhammad Zafar Mengal ArticlesDocumento4 páginasArgh - Ms.id.555581, DR Muhammad Zafar Mengal ArticlesMuhammad Zafar MengalAún no hay calificaciones
- Wormuth 2006Documento12 páginasWormuth 2006DH SiriruiAún no hay calificaciones
- DTSCH Arztebl Int-109-0617Documento7 páginasDTSCH Arztebl Int-109-0617Carlos PalaciosAún no hay calificaciones
- Oesophagocoloplasty For Corrosive Oesophageal Stricture: AbstractDocumento12 páginasOesophagocoloplasty For Corrosive Oesophageal Stricture: AbstractSpandan KadamAún no hay calificaciones
- B - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Documento16 páginasB - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Battousaih1Aún no hay calificaciones
- Laparoscopic Gastrointestinal SurgeryDocumento22 páginasLaparoscopic Gastrointestinal SurgeryRoxana BoloagaAún no hay calificaciones
- CholecystectomyDocumento2 páginasCholecystectomyHiylie MartinezAún no hay calificaciones
- Cholelithiasis Treatment & ManagementDocumento8 páginasCholelithiasis Treatment & ManagementRayhanun MardhatillahAún no hay calificaciones
- ZollingerDocumento5 páginasZollingerSantiago Xicotencatl MendezAún no hay calificaciones
- Ureteral ReconstructionDocumento6 páginasUreteral ReconstructiongumAún no hay calificaciones
- Assessment TN MasrukhiDocumento3 páginasAssessment TN MasrukhiAngger SatriaAún no hay calificaciones
- Urushihara 10.1007 s00383-015-3779-8Documento4 páginasUrushihara 10.1007 s00383-015-3779-8CherAún no hay calificaciones
- Case ReportDocumento5 páginasCase ReportAmmar magdyAún no hay calificaciones
- Surgery Illustrated - Focus - Tapering of The MegaureterDocumento5 páginasSurgery Illustrated - Focus - Tapering of The MegauretermoetazAún no hay calificaciones
- Safe CholecystectomyDocumento60 páginasSafe CholecystectomyCarlos Reyes100% (1)
- Equine Abdominal SurgeryDocumento76 páginasEquine Abdominal SurgeryasheneyAún no hay calificaciones
- PancreaticoduodenectomyDocumento2 páginasPancreaticoduodenectomymarkfernandoeAún no hay calificaciones
- Bakshi 2017Documento7 páginasBakshi 2017DH SiriruiAún no hay calificaciones
- Closure of Loop Ileostomy Potentially ADocumento7 páginasClosure of Loop Ileostomy Potentially Ashah hassaanAún no hay calificaciones
- Cholecystectomy: Cholecystectomy (Pronounced / Kɒləsɪs Tɛktəmi/, Plural: Cholecystectomies) Is TheDocumento3 páginasCholecystectomy: Cholecystectomy (Pronounced / Kɒləsɪs Tɛktəmi/, Plural: Cholecystectomies) Is Thejosias_jorgio1Aún no hay calificaciones
- Cholecystectomy: Navigation SearchDocumento4 páginasCholecystectomy: Navigation SearchMohammed OmerAún no hay calificaciones
- 54.the Gallbladder and Bile DuctsDocumento19 páginas54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondAún no hay calificaciones
- T Tube by Daldoul2012Documento7 páginasT Tube by Daldoul2012Suhenri SiahaanAún no hay calificaciones
- Sleeve-Gastrectomy 2011 BrethauerDocumento15 páginasSleeve-Gastrectomy 2011 BrethauerDavid Schnettler RodriguezAún no hay calificaciones
- Overview: 1.1 BackgroundDocumento12 páginasOverview: 1.1 BackgroundAndika Dwiputra DjajaAún no hay calificaciones
- Choice of Enterostoma: Feeding JejunostomyDocumento4 páginasChoice of Enterostoma: Feeding JejunostomyFikranaya SalimAún no hay calificaciones
- International Journal of Surgery Case ReportsDocumento5 páginasInternational Journal of Surgery Case ReportsJuan Eduardo Rios RodriguezAún no hay calificaciones
- Colonic Interposition For Benign DiseaseDocumento18 páginasColonic Interposition For Benign DiseaseOhana S.Aún no hay calificaciones
- Open Cholecystectomy ReportDocumento7 páginasOpen Cholecystectomy ReportjosephcloudAún no hay calificaciones
- BiliaryDocumento41 páginasBiliaryayundyawibowoAún no hay calificaciones
- Colostomy & Colostomy CareDocumento56 páginasColostomy & Colostomy Careapi-3722454100% (31)
- Cirugía y Cirujanos: Gallstone Ileus After Endoscopic Retrograde CholangiopancreatographyDocumento4 páginasCirugía y Cirujanos: Gallstone Ileus After Endoscopic Retrograde CholangiopancreatographyMuhammad Fuad MahfudAún no hay calificaciones
- Partial CholelithiasisDocumento4 páginasPartial CholelithiasisSyamsulBahriANAún no hay calificaciones
- Final EditDocumento43 páginasFinal EditMary Rose LinatocAún no hay calificaciones
- Laparoscopic Splenectomy: Standardized ApproachDocumento9 páginasLaparoscopic Splenectomy: Standardized ApproachLauraAún no hay calificaciones
- Cholecystectomy (: Laparoscopic GallstonesDocumento4 páginasCholecystectomy (: Laparoscopic GallstonesAlexia BatungbacalAún no hay calificaciones
- 012011SCNA3Documento14 páginas012011SCNA3mariafmhAún no hay calificaciones
- Video DigestDocumento18 páginasVideo Digestsahirwar02Aún no hay calificaciones
- Intestinal Stomas PDFDocumento12 páginasIntestinal Stomas PDFRye Asri Mashudy Dhasry100% (1)
- Blumgart Anastomosis For Pancreaticojejunostomy Minimizes Severe Complications After Pancreatic Head ResectionDocumento10 páginasBlumgart Anastomosis For Pancreaticojejunostomy Minimizes Severe Complications After Pancreatic Head ResectionRegina UgarteAún no hay calificaciones
- Buccal Mucosa Urethroplasty For Adult Urethral Strictures - PMCDocumento13 páginasBuccal Mucosa Urethroplasty For Adult Urethral Strictures - PMCEllya Syahfitri 2108125983Aún no hay calificaciones
- IPSS QuizDocumento2 páginasIPSS QuizmoetazAún no hay calificaciones
- Uro Embryology Cunha 2004Documento16 páginasUro Embryology Cunha 2004moetazAún no hay calificaciones
- Surgery Illustrated - Focus - Tapering of The MegaureterDocumento5 páginasSurgery Illustrated - Focus - Tapering of The MegauretermoetazAún no hay calificaciones
- Anatomy of The Anterior Abdominal Wall & Groin PDFDocumento4 páginasAnatomy of The Anterior Abdominal Wall & Groin PDFmoetazAún no hay calificaciones
- Rusch Urology BroschureDocumento72 páginasRusch Urology BroschuremoetazAún no hay calificaciones
- Post Graduate 2013Documento4 páginasPost Graduate 2013moetazAún no hay calificaciones
- Modified Gibson Incision - WikipediaDocumento1 páginaModified Gibson Incision - WikipediamoetazAún no hay calificaciones
- TJW Neurogenic BladderDocumento8 páginasTJW Neurogenic BladdermoetazAún no hay calificaciones
- Nej Mic M 1308004Documento1 páginaNej Mic M 1308004moetazAún no hay calificaciones
- Cadmium in VXDocumento12 páginasCadmium in VXmoetazAún no hay calificaciones
- Active Surveillance For Prostate Cancer AUA Update 33 2008Documento8 páginasActive Surveillance For Prostate Cancer AUA Update 33 2008moetazAún no hay calificaciones
- Digital Rectal Examination (Prostate Exam) - WWW - Urology-TextbookDocumento2 páginasDigital Rectal Examination (Prostate Exam) - WWW - Urology-TextbookmoetazAún no hay calificaciones
- Histo Lab Exercise #14Documento4 páginasHisto Lab Exercise #14Gela ReyesAún no hay calificaciones
- Cholecystectomy (Gallbladder Removal)Documento6 páginasCholecystectomy (Gallbladder Removal)Katleen Calang AlagAún no hay calificaciones
- MD II Material Pentru 10.03.2020Documento4 páginasMD II Material Pentru 10.03.2020Irina Panciu StefanAún no hay calificaciones
- Assignment Structure of Oral CavityDocumento4 páginasAssignment Structure of Oral CavityNarjis BatoolAún no hay calificaciones
- Peptic Ulcer LP PDF FreeDocumento8 páginasPeptic Ulcer LP PDF FreeAвнιѕнєĸ BαjpαιAún no hay calificaciones
- Gastrointestinal: Metastatic Melanoma of The TractDocumento5 páginasGastrointestinal: Metastatic Melanoma of The TractCristi PopescuAún no hay calificaciones
- Lab 13 Digestive SystemDocumento11 páginasLab 13 Digestive SystemMary Dominique D. TambienAún no hay calificaciones
- Las Science 8 m1Documento9 páginasLas Science 8 m1Diamond CrsktAún no hay calificaciones
- The Microbiota in Cirrhosis and Its Role in Hepatic Decompensation. 2020Documento15 páginasThe Microbiota in Cirrhosis and Its Role in Hepatic Decompensation. 2020mafe.z.solarte87Aún no hay calificaciones
- Quiz Biology Pre Igcse 3Documento17 páginasQuiz Biology Pre Igcse 3eric sivaneshAún no hay calificaciones
- Cholecystitis BelgradeDocumento52 páginasCholecystitis BelgradeLazar VučetićAún no hay calificaciones
- Lesions Portal Gastritis Congestive Gastropathy?: Gastric in Hypertension: InflammatoryDocumento7 páginasLesions Portal Gastritis Congestive Gastropathy?: Gastric in Hypertension: InflammatoryAnisa SafutriAún no hay calificaciones
- What Is Colonoscopy and Its PurposeDocumento6 páginasWhat Is Colonoscopy and Its PurposeGrape JuiceAún no hay calificaciones
- GI Tract Histology SummaryDocumento5 páginasGI Tract Histology SummaryFluffy_iceAún no hay calificaciones
- Repuestos MaterialDocumento18 páginasRepuestos MaterialCristhian Andree Lucar MonzonAún no hay calificaciones
- Hubungan Asupan Serat Makanan Dan Cairan Dengan Kejadian Konstipasi Fungsional Pada Remaja Di Sma Kesatrian 1 SemarangDocumento10 páginasHubungan Asupan Serat Makanan Dan Cairan Dengan Kejadian Konstipasi Fungsional Pada Remaja Di Sma Kesatrian 1 SemarangHanifAún no hay calificaciones
- Hepatic, Pancreatic, and Rare Gastrointestinal Complications of Immune Checkpoint Inhibitor Therapy - UpToDateDocumento29 páginasHepatic, Pancreatic, and Rare Gastrointestinal Complications of Immune Checkpoint Inhibitor Therapy - UpToDatemayteveronica1000Aún no hay calificaciones
- GIT Abnormality in Infant/Children On Radiology Imaging Which Need Surgery CorrectionDocumento48 páginasGIT Abnormality in Infant/Children On Radiology Imaging Which Need Surgery Correctiondr fikriAún no hay calificaciones
- Growth Inhibition of Probiotics On The Growth of Streptococcus MutansDocumento4 páginasGrowth Inhibition of Probiotics On The Growth of Streptococcus MutansSi EllaAún no hay calificaciones
- QT4 - Science 8Documento3 páginasQT4 - Science 8joseph mampustiAún no hay calificaciones
- GIDocumento196 páginasGIswagmasterAún no hay calificaciones
- Biology Grade 8-Quarter 4: He Stomach Muscles Mix The Food and Liquid With Digestive JuicesDocumento6 páginasBiology Grade 8-Quarter 4: He Stomach Muscles Mix The Food and Liquid With Digestive Juicesleah jane malinaoAún no hay calificaciones
- Biliary AtresiaDocumento25 páginasBiliary Atresiajulius billiAún no hay calificaciones
- Ceklist Harian Alat Laparotomy Merk RudolfDocumento4 páginasCeklist Harian Alat Laparotomy Merk RudolfDiahAún no hay calificaciones
- 11th Zoology Ps Answer Key For Quarterly Exam 2019 Question Paper Shri Krishna English MediumDocumento11 páginas11th Zoology Ps Answer Key For Quarterly Exam 2019 Question Paper Shri Krishna English Mediumsri thamizhanAún no hay calificaciones
- CP On Calculous CholelithiasisDocumento102 páginasCP On Calculous Cholelithiasiskathy100% (3)
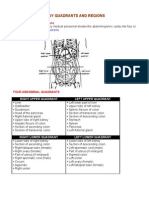
- Organs in The Body Quadrants and RegionsDocumento3 páginasOrgans in The Body Quadrants and RegionsDavid HosamAún no hay calificaciones
- PHS 222/225 Git PhysiologyDocumento32 páginasPHS 222/225 Git PhysiologyDurchessAún no hay calificaciones
- Colostomy Care ReviseDocumento6 páginasColostomy Care ReviseMeryl Mae RamosAún no hay calificaciones
- Colonoscopy: Dr. Aditya Hans Suwignjo, M.HDocumento18 páginasColonoscopy: Dr. Aditya Hans Suwignjo, M.HRenaa PujiiAún no hay calificaciones