También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- F Table 1Documento8 páginasF Table 1Talha IdreesAún no hay calificaciones
- 8.-ANATOMY and Physiology GIDocumento12 páginas8.-ANATOMY and Physiology GIAngelica Cassandra VillenaAún no hay calificaciones
- Elective ShockDocumento40 páginasElective ShockAngelica Cassandra VillenaAún no hay calificaciones
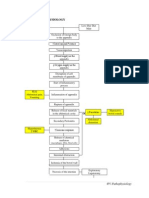
- Appendicitis PathophysiologyDocumento4 páginasAppendicitis PathophysiologyAngelica Cassandra VillenaAún no hay calificaciones
- Sepsis in Older PatientsDocumento8 páginasSepsis in Older PatientsFajar WasilahAún no hay calificaciones
- Marcos Administration: Capv, Bsa 2-6Documento2 páginasMarcos Administration: Capv, Bsa 2-6Angelica Cassandra VillenaAún no hay calificaciones
- Lcohol: Key FactsDocumento4 páginasLcohol: Key FactsAngelica Cassandra VillenaAún no hay calificaciones
- Psychiatric Observation A Skill Worth DevelopingDocumento30 páginasPsychiatric Observation A Skill Worth DevelopingAngelica Cassandra VillenaAún no hay calificaciones
- Sustainability in NursingDocumento18 páginasSustainability in NursingAngelica Cassandra VillenaAún no hay calificaciones
- Mental Health ActDocumento9 páginasMental Health ActAngelica Cassandra Villena100% (1)
- JanuaryDocumento2 páginasJanuaryAngelica Cassandra VillenaAún no hay calificaciones
- Drug Study: Cavite State University (Cvsu)Documento2 páginasDrug Study: Cavite State University (Cvsu)Angelica Cassandra VillenaAún no hay calificaciones
- BibliographyDocumento2 páginasBibliographyAngelica Cassandra VillenaAún no hay calificaciones
- Physical Activity: Key FactsDocumento4 páginasPhysical Activity: Key FactsAngelica Cassandra VillenaAún no hay calificaciones
- Drug Study: Don Severino Delas Alas Campus Indang, Cavite (046) 4150-010 / 4150-011 (046) 4150-012Documento1 páginaDrug Study: Don Severino Delas Alas Campus Indang, Cavite (046) 4150-010 / 4150-011 (046) 4150-012Angelica Cassandra VillenaAún no hay calificaciones
- United States of America National AnthemDocumento1 páginaUnited States of America National AnthemGaco Costa RicaAún no hay calificaciones
- Lcohol: Key FactsDocumento4 páginasLcohol: Key FactsAngelica Cassandra VillenaAún no hay calificaciones
- EvaluationDocumento2 páginasEvaluationAngelica Cassandra VillenaAún no hay calificaciones
- Article 5Documento21 páginasArticle 5Angelica Cassandra VillenaAún no hay calificaciones
- Art 8Documento27 páginasArt 8Angelica Cassandra VillenaAún no hay calificaciones
- AspirinDocumento2 páginasAspirinAngelica Cassandra VillenaAún no hay calificaciones
- CETIRIZINEDocumento2 páginasCETIRIZINEAngelica Cassandra Villena100% (10)
- Mefenamic AcidDocumento3 páginasMefenamic AcidAngelica Cassandra VillenaAún no hay calificaciones
- Department of Health: History, Policy, Budget, Programs For HealthDocumento57 páginasDepartment of Health: History, Policy, Budget, Programs For HealthAngelica Cassandra VillenaAún no hay calificaciones
- CEFTRIAZONEDocumento2 páginasCEFTRIAZONEAngelica Cassandra VillenaAún no hay calificaciones
- CEFRADINEDocumento2 páginasCEFRADINEAngelica Cassandra VillenaAún no hay calificaciones
- CefoxitinDocumento3 páginasCefoxitinAngelica Cassandra VillenaAún no hay calificaciones
- HISTORYDocumento3 páginasHISTORYAngelica Cassandra VillenaAún no hay calificaciones
- AspirinDocumento2 páginasAspirinAngelica Cassandra VillenaAún no hay calificaciones
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (120)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2101)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Bipolar I Disorder Case ExampleDocumento6 páginasBipolar I Disorder Case ExampleGrape JuiceAún no hay calificaciones
- A Network Meta-Analysis On The Effects of Information Technology Application On Preoperative Anxiety of PatientsDocumento7 páginasA Network Meta-Analysis On The Effects of Information Technology Application On Preoperative Anxiety of PatientsInternational Journal of Application or Innovation in Engineering & ManagementAún no hay calificaciones
- (Therapy in Practice Series) Rosemary Gravell, Jenny France (Auth.) - Speech and Communication Problems in Psychiatry (1991, Springer US) PDFDocumento364 páginas(Therapy in Practice Series) Rosemary Gravell, Jenny France (Auth.) - Speech and Communication Problems in Psychiatry (1991, Springer US) PDFmelike50% (2)
- Family Nursing Care Plan SeizuresDocumento3 páginasFamily Nursing Care Plan SeizuresClaire AlcantaraAún no hay calificaciones
- Basic TB FactsDocumento8 páginasBasic TB FactshatemfaroukAún no hay calificaciones
- Don Mottin - Stage Hypnosis - Class HandoutsDocumento46 páginasDon Mottin - Stage Hypnosis - Class HandoutsRaphael Maurin100% (2)
- Anemia PPT 3 Nov 2014Documento60 páginasAnemia PPT 3 Nov 2014Susi DesmaryaniAún no hay calificaciones
- Evaluation of Passive Stretching in The Hamstrings FlexibilityDocumento10 páginasEvaluation of Passive Stretching in The Hamstrings FlexibilitylinaAún no hay calificaciones
- Medical Kit Components EandEDocumento54 páginasMedical Kit Components EandETroy Ashcraft100% (2)
- Handbook: For Clinical Management of DengueDocumento124 páginasHandbook: For Clinical Management of DengueraattaiAún no hay calificaciones
- Pelvic Inflammatory DiseaseDocumento34 páginasPelvic Inflammatory DiseaseOhunakin AfolabiAún no hay calificaciones
- CPD Questions For Volume 21 Issue 3Documento4 páginasCPD Questions For Volume 21 Issue 3KeeranmayeeishraAún no hay calificaciones
- Pediatric LeukemiasDocumento42 páginasPediatric LeukemiasslyfoxkittyAún no hay calificaciones
- Aripiprazole - Mechanism of Action, Clinical Efficacy and Side EffectsDocumento10 páginasAripiprazole - Mechanism of Action, Clinical Efficacy and Side EffectsRuben Del CidAún no hay calificaciones
- Therapy ManualDocumento52 páginasTherapy ManualcrisAún no hay calificaciones
- NYCDEP 2007 503 Annual ReportDocumento584 páginasNYCDEP 2007 503 Annual ReportNYC SludgeAún no hay calificaciones
- Fibula Stress Fractures: A Treatment Review: Iftach Hetsroni, MD, and Gideon Mann, MDDocumento3 páginasFibula Stress Fractures: A Treatment Review: Iftach Hetsroni, MD, and Gideon Mann, MDJamaluddin HaikhahAún no hay calificaciones
- Dan CV WordDocumento4 páginasDan CV WorddsnavarretteAún no hay calificaciones
- Sop Chlorine GasDocumento3 páginasSop Chlorine GashmtlionAún no hay calificaciones
- ResumeDocumento4 páginasResumeapi-283952616Aún no hay calificaciones
- Curosurf 120mg / Vial Endotracheopulmonary Instillation Suspension Curosurf 240mg / Vial Endotracheopulmonary Instillation SuspensionDocumento2 páginasCurosurf 120mg / Vial Endotracheopulmonary Instillation Suspension Curosurf 240mg / Vial Endotracheopulmonary Instillation SuspensionHerlinsye PurimahuaAún no hay calificaciones
- HeatStress NEWDocumento33 páginasHeatStress NEWJeffrey Arandia100% (1)
- Allergy Test PapersDocumento5 páginasAllergy Test PapersDaniel MoncadaAún no hay calificaciones
- Is An Ancient Disease That Causes Permanent Physical Disability AmongDocumento6 páginasIs An Ancient Disease That Causes Permanent Physical Disability Amongkian5Aún no hay calificaciones
- Pontalis, J. B. (2014) - No, Twice NoDocumento19 páginasPontalis, J. B. (2014) - No, Twice NocabaretdadaAún no hay calificaciones
- Buset Na ResearchDocumento5 páginasBuset Na Researchmk soberanoAún no hay calificaciones
- Future PharmaDocumento40 páginasFuture Pharmaet43864Aún no hay calificaciones
- Drug Benefit ListDocumento221 páginasDrug Benefit ListPharmaruthiAún no hay calificaciones
- Murtagh's Practice Tips, 6th EditionDocumento281 páginasMurtagh's Practice Tips, 6th EditionAishath MohamedAún no hay calificaciones
- Medicines, 6th EdDocumento609 páginasMedicines, 6th EdNguyễn Sanh Luật50% (2)