También podría gustarte
- Clinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3De EverandClinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3Calificación: 5 de 5 estrellas5/5 (1)
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsDe EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsCalificación: 5 de 5 estrellas5/5 (9)
- Adjupanrix LeafletDocumento42 páginasAdjupanrix LeafletEllaAún no hay calificaciones
- Comirnaty Epar Product Information - enDocumento536 páginasComirnaty Epar Product Information - enManaila GabrielAún no hay calificaciones
- Adult ScheduleDocumento3 páginasAdult ScheduledrmanojvimalAún no hay calificaciones
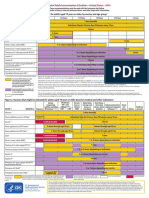
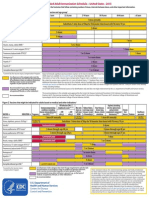
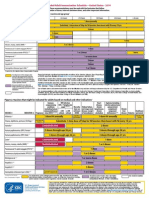
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocumento2 páginasFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasAún no hay calificaciones
- Cervarix 2018Documento26 páginasCervarix 2018Jacob PaglinawanAún no hay calificaciones
- Annex I Summary of Product CharacteristicsDocumento33 páginasAnnex I Summary of Product CharacteristicsVimala BohoAún no hay calificaciones
- Gardasil LeafletDocumento51 páginasGardasil LeafletEllaAún no hay calificaciones
- Adult Combined ScheduleDocumento5 páginasAdult Combined SchedulelcmurilloAún no hay calificaciones
- Adult Immunization ScheduleDocumento3 páginasAdult Immunization ScheduleBryan Mae H. DegorioAún no hay calificaciones
- Adult Pocafeket SizeDocumento2 páginasAdult Pocafeket SizedadfAún no hay calificaciones
- Adult ScheduleDocumento3 páginasAdult SchedulelcmurilloAún no hay calificaciones
- ImmunizationDocumento40 páginasImmunizationHilyaJae-heeAún no hay calificaciones
- Gardasil 9 LeafletDocumento46 páginasGardasil 9 LeafletEllaAún no hay calificaciones
- Reg 174 Information For Uk Healthcare ProfessionalsDocumento11 páginasReg 174 Information For Uk Healthcare ProfessionalsSelenaAún no hay calificaciones
- SOMis AdminDocumento14 páginasSOMis AdminLINGGA DEWIAún no hay calificaciones
- Qdenga Epar Product Information enDocumento47 páginasQdenga Epar Product Information enNovrina Wahidah RestiAún no hay calificaciones
- Annex I Summary of Product CharacteristicsDocumento34 páginasAnnex I Summary of Product CharacteristicsgladioAún no hay calificaciones
- MY VaxigripTetra NH (0522)Documento14 páginasMY VaxigripTetra NH (0522)prasanthgkrishnan1402Aún no hay calificaciones
- Summary of Recommendations For Child Teen Immunization: (Age Birth Through 18 Years)Documento5 páginasSummary of Recommendations For Child Teen Immunization: (Age Birth Through 18 Years)Annie AnnaAún no hay calificaciones
- Comirnaty Epar Product Information - enDocumento34 páginasComirnaty Epar Product Information - enAuraAún no hay calificaciones
- Summary of Recommendations For Adult Immunization: (Age 19 Years and Older)Documento5 páginasSummary of Recommendations For Adult Immunization: (Age 19 Years and Older)Hannah Caburian RemoAún no hay calificaciones
- EMA - Pandemrix® (Vaccin A H1N1 - GSK)Documento37 páginasEMA - Pandemrix® (Vaccin A H1N1 - GSK)Tiffany TorresAún no hay calificaciones
- Cervarix LeafletDocumento83 páginasCervarix LeafletEllaAún no hay calificaciones
- Annex I Summary of Product CharacteristicsDocumento33 páginasAnnex I Summary of Product CharacteristicsMohamed AllamAún no hay calificaciones
- Annex I Summary of Product CharacteristicsDocumento33 páginasAnnex I Summary of Product CharacteristicsEva DominguezAún no hay calificaciones
- Splenectomy: DisclaimerDocumento5 páginasSplenectomy: DisclaimerMimi FatinAún no hay calificaciones
- Annex I Summary of Product CharacteristicsDocumento34 páginasAnnex I Summary of Product CharacteristicsLaura RačytėAún no hay calificaciones
- Covid 19 Vaccine Astra ZenecainjDocumento17 páginasCovid 19 Vaccine Astra ZenecainjGlowstarAún no hay calificaciones
- Annex I Summary of Product CharacteristicsDocumento37 páginasAnnex I Summary of Product Characteristicstanasa adrianAún no hay calificaciones
- Kiss Covid VaccinationsDocumento4 páginasKiss Covid VaccinationsMohamed Ali KalathingalAún no hay calificaciones
- Adult Schedule 11x17Documento2 páginasAdult Schedule 11x17lcmurilloAún no hay calificaciones
- Adult Combined ScheduleDocumento5 páginasAdult Combined ScheduleAwal Safar MAún no hay calificaciones
- ACC Qdenga SMPCDocumento18 páginasACC Qdenga SMPCAngsamerahAún no hay calificaciones
- Influvac: New Zealand Data SheetDocumento7 páginasInfluvac: New Zealand Data SheetAtthapu ThirupathaiahAún no hay calificaciones
- Immunization ScheduleDocumento2 páginasImmunization ScheduleTracy100% (1)
- Varilrix Serbuk Injeksi 2000 PFU, Dosis - Vaksin Varisela - Zoster - DKI9676701044A1 - 2018 - 3Documento8 páginasVarilrix Serbuk Injeksi 2000 PFU, Dosis - Vaksin Varisela - Zoster - DKI9676701044A1 - 2018 - 3rianaAún no hay calificaciones
- Practice Changing UpDates - UpToDateDocumento13 páginasPractice Changing UpDates - UpToDatemayteveronica1000Aún no hay calificaciones
- Reg 174 Information For Uk Healthcare ProfessionalsDocumento13 páginasReg 174 Information For Uk Healthcare ProfessionalsIce BallAún no hay calificaciones
- SPC COMIRNATY BA1 Bivalent 12+ YearsDocumento23 páginasSPC COMIRNATY BA1 Bivalent 12+ YearsMaressa BerbetAún no hay calificaciones
- Moderna Fact Sheet Pi Providers CleanDocumento35 páginasModerna Fact Sheet Pi Providers CleanEvropej “Evy” AlimiAún no hay calificaciones
- Ensayos Clínicos Vacuna COVID-RNAmDocumento278 páginasEnsayos Clínicos Vacuna COVID-RNAmGustavo Benavides LatorreAún no hay calificaciones
- Vaccine Timing CDCDocumento40 páginasVaccine Timing CDCanindita.prasidha.parameswariAún no hay calificaciones
- V.3 21195 Sinopharm Vaccine Explainer 24Documento6 páginasV.3 21195 Sinopharm Vaccine Explainer 24Mohammad Hisham BhawpalAún no hay calificaciones
- COVID-19 MRNA Vaccine MRNA-1273 ModernaDocumento4 páginasCOVID-19 MRNA Vaccine MRNA-1273 ModernawalkrogAún no hay calificaciones
- Adult ScheduleDocumento3 páginasAdult ScheduleerilarchiAún no hay calificaciones
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Documento4 páginasSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)gyna_2002Aún no hay calificaciones
- Pfizer BioNTech and Comirnaty Product Information For HCPDocumento20 páginasPfizer BioNTech and Comirnaty Product Information For HCPJuan PaoloAún no hay calificaciones
- 1 CombineDocumento726 páginas1 CombineSong Hành Vạn KiếpAún no hay calificaciones
- M M Rvaxpro ProspectDocumento57 páginasM M Rvaxpro ProspectNicoleta CiobotarAún no hay calificaciones
- Influenza Antiviral Medications: A Summary For CliniciansDocumento6 páginasInfluenza Antiviral Medications: A Summary For CliniciansSachin S RaneAún no hay calificaciones
- IZSchedule0 6yrsDocumento1 páginaIZSchedule0 6yrsKaty ForemanAún no hay calificaciones
- Annex I Summary of Product CharacteristicsDocumento35 páginasAnnex I Summary of Product Characteristicsmihaela vlad100% (1)
- Vaxzevria Previously Covid 19 Vaccine Astrazeneca Epar Product Information enDocumento37 páginasVaxzevria Previously Covid 19 Vaccine Astrazeneca Epar Product Information enEthrigan DaemonicusAún no hay calificaciones
- Antiviral Summary Clinicians InfluenzaDocumento8 páginasAntiviral Summary Clinicians InfluenzaSylvia GonzalezAún no hay calificaciones
- Annex I Summary of Product CharacteristicsDocumento55 páginasAnnex I Summary of Product CharacteristicsEllaAún no hay calificaciones
- Neutropenic Fever Empiric TherapyDocumento5 páginasNeutropenic Fever Empiric TherapyRominaPulvermüllerSalvatierraAún no hay calificaciones
- Brivaracetam-50mg TabletDocumento10 páginasBrivaracetam-50mg TabletMd. Abdur RahmanAún no hay calificaciones
- Reg 174 Information For Uk Healthcare ProfessionalsDocumento11 páginasReg 174 Information For Uk Healthcare ProfessionalsEDUARDO MachadoAún no hay calificaciones
- Virology of Human Papillomavirus Infections and The Link To CancerDocumento10 páginasVirology of Human Papillomavirus Infections and The Link To Canceralejandro fernandezAún no hay calificaciones
- Cervical and Vaginal CytologyDocumento18 páginasCervical and Vaginal Cytologyalejandro fernandezAún no hay calificaciones
- Cervical Intraepithelial NeoplasiaDocumento16 páginasCervical Intraepithelial Neoplasiaalejandro fernandezAún no hay calificaciones
- Condylomata AcuminataDocumento10 páginasCondylomata Acuminataalejandro fernandezAún no hay calificaciones
- Carcinoma of PenisDocumento13 páginasCarcinoma of Penisalejandro fernandezAún no hay calificaciones
- digiPHONENT UG enDocumento44 páginasdigiPHONENT UG enIrving Javier Leal OrtizAún no hay calificaciones
- Parle G ReportDocumento7 páginasParle G ReportnikhilAún no hay calificaciones
- Data Sheet HFE-7000 Prod SpecDocumento6 páginasData Sheet HFE-7000 Prod Specsshaffer_9Aún no hay calificaciones
- Fischer General-CatalogueDocumento108 páginasFischer General-Cataloguebo cephusAún no hay calificaciones
- Security Officer Part Time in Orange County CA Resume Robert TalleyDocumento2 páginasSecurity Officer Part Time in Orange County CA Resume Robert TalleyRobertTalleyAún no hay calificaciones
- Respirator LangmanDocumento10 páginasRespirator LangmanSavu MalinaAún no hay calificaciones
- PHC Visit: Chandreswor Primary Health Care Centre: TH TH TH THDocumento6 páginasPHC Visit: Chandreswor Primary Health Care Centre: TH TH TH THShashanka PoudelAún no hay calificaciones
- G1 CurvedDocumento16 páginasG1 CurvedElbert Ryan OcampoAún no hay calificaciones
- 19.-Solid Waste TreatmentDocumento108 páginas19.-Solid Waste TreatmentShaira Dale100% (1)
- Gene SileningDocumento30 páginasGene SileningSajjad AhmadAún no hay calificaciones
- Abrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition Test BankDocumento6 páginasAbrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition Test BankWilliam Nakken100% (28)
- Osmotic Power Generation: Prepared byDocumento16 páginasOsmotic Power Generation: Prepared byPritam MishraAún no hay calificaciones
- Kristen Swanson's Theory of CaringDocumento12 páginasKristen Swanson's Theory of CaringAlexandria David50% (2)
- Cruz v. CA - G.R. No. 122445 - November 18, 1997 - DIGESTDocumento2 páginasCruz v. CA - G.R. No. 122445 - November 18, 1997 - DIGESTAaron Ariston80% (5)
- NEWS BD RAE Letter of Intent-Press-release1Documento2 páginasNEWS BD RAE Letter of Intent-Press-release1Anthony D.Aún no hay calificaciones
- Turbo Lab 1Documento10 páginasTurbo Lab 1Seng SoonAún no hay calificaciones
- Prednisolone Versus Dexamethasone For Croup: A Randomized Controlled TrialDocumento11 páginasPrednisolone Versus Dexamethasone For Croup: A Randomized Controlled TrialA Joel ZjAún no hay calificaciones
- 4:30:21 PaystubDocumento1 página4:30:21 PaystubRhoderlande JosephAún no hay calificaciones
- Principles in Biochemistry (SBK3013)Documento3 páginasPrinciples in Biochemistry (SBK3013)Leena MuniandyAún no hay calificaciones
- Report of Initial / Annual / Intermediate / Renewal / General Examination SurveyDocumento9 páginasReport of Initial / Annual / Intermediate / Renewal / General Examination SurveyJagjit SinghAún no hay calificaciones
- Ocean StarDocumento36 páginasOcean Starrobertshepard1967Aún no hay calificaciones
- Jose de Villa National School: Home Visitation FormDocumento3 páginasJose de Villa National School: Home Visitation FormNoli AsuroAún no hay calificaciones
- Victron Orion-Tr - Smart - DC-DC - Charger-Manual Non IsolatedDocumento19 páginasVictron Orion-Tr - Smart - DC-DC - Charger-Manual Non IsolatedThomist AquinasAún no hay calificaciones
- Evaluation and Comparison of Highly Soluble Sodium Stearyl Fumarate With Other Lubricants in VitroDocumento8 páginasEvaluation and Comparison of Highly Soluble Sodium Stearyl Fumarate With Other Lubricants in VitroSvirskaitė LaurynaAún no hay calificaciones
- 2nd Year HEROES SUMMARIESDocumento4 páginas2nd Year HEROES SUMMARIESMustafa NizamiAún no hay calificaciones
- Refuse Chute PPT 01Documento11 páginasRefuse Chute PPT 01sanika shindeAún no hay calificaciones
- Key Nursing SkillsDocumento359 páginasKey Nursing Skillsmordanga100% (6)
- FACSDocumento8 páginasFACSKarthick ThiyagarajanAún no hay calificaciones
- RSA 12 - Laser Attacks Safety GuidelinesDocumento19 páginasRSA 12 - Laser Attacks Safety Guidelinesrona putriAún no hay calificaciones
- Flaxseed Paper PublishedDocumento4 páginasFlaxseed Paper PublishedValentina GarzonAún no hay calificaciones