También podría gustarte
- New and Emerging Issues in Latinx HealthDe EverandNew and Emerging Issues in Latinx HealthAirín D. MartínezAún no hay calificaciones
- 09 ARTI Ryan 417 426Documento10 páginas09 ARTI Ryan 417 426Sifra Turu AlloAún no hay calificaciones
- BMC Health Services Research: Digging Deeper: Quality of Patient-Provider Communication Across Hispanic SubgroupsDocumento8 páginasBMC Health Services Research: Digging Deeper: Quality of Patient-Provider Communication Across Hispanic SubgroupsTitan LinggastiwiAún no hay calificaciones
- 10.1007@s40471 017 0111 2Documento11 páginas10.1007@s40471 017 0111 2eekkaa.ecAún no hay calificaciones
- Research Proposal FinalDocumento13 páginasResearch Proposal Finalapi-326037307Aún no hay calificaciones
- NIH Public Access: Author ManuscriptDocumento12 páginasNIH Public Access: Author ManuscriptjimakosjpAún no hay calificaciones
- Latino ManualDocumento69 páginasLatino ManualstthomasAún no hay calificaciones
- University of California PostprintsDocumento37 páginasUniversity of California PostprintsPilar Galiano CruzAún no hay calificaciones
- For WEB - ELDER ABUSE Wrap Is Edited Below and in P For MONDAY AirDocumento7 páginasFor WEB - ELDER ABUSE Wrap Is Edited Below and in P For MONDAY AirEric ZassenhausAún no hay calificaciones
- Low Latino Immunization Rates E-Portfolio 3Documento7 páginasLow Latino Immunization Rates E-Portfolio 3api-300678072Aún no hay calificaciones
- Desigualdad Socioeconómica y Salud en MéxicoDocumento12 páginasDesigualdad Socioeconómica y Salud en MéxicoAmisadai LugoAún no hay calificaciones
- Prevalence of Hepatitis B Virus Infection and Related Risk Factors in A Rural Community of MexicoDocumento5 páginasPrevalence of Hepatitis B Virus Infection and Related Risk Factors in A Rural Community of MexicoEmmanuel LawerAún no hay calificaciones
- Tribally Driven AIDS Health Services Partnerships - Evidence-Based Meets Culture-Centered Interventions-2Documento20 páginasTribally Driven AIDS Health Services Partnerships - Evidence-Based Meets Culture-Centered Interventions-2bonduranAún no hay calificaciones
- Behavioral Sciences: The Link Between Mastery and Depression Among Black Adolescents Ethnic and Gender DifferencesDocumento13 páginasBehavioral Sciences: The Link Between Mastery and Depression Among Black Adolescents Ethnic and Gender DifferencesArturo Chávez FloresAún no hay calificaciones
- Hispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research LiteratureDocumento27 páginasHispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research LiteratureUrbanYouthJusticeAún no hay calificaciones
- Socioeconomic, Cultural, and Behavioral Factors Affecting Hispanic Health OutcomesDocumento27 páginasSocioeconomic, Cultural, and Behavioral Factors Affecting Hispanic Health OutcomesLLLJJJAún no hay calificaciones
- Reported Benefits of Participation in A Research StudyDocumento6 páginasReported Benefits of Participation in A Research StudyAaron SAún no hay calificaciones
- Altin Kukic - Final Research ReportDocumento20 páginasAltin Kukic - Final Research ReportAltin KukicAún no hay calificaciones
- Culture Nihms741987Documento17 páginasCulture Nihms741987dwiputra1996Aún no hay calificaciones
- Valdez 2021. Making Sense of Chagas Disease Among Mexican Immigrants in CaliforniaDocumento15 páginasValdez 2021. Making Sense of Chagas Disease Among Mexican Immigrants in CaliforniaAlbaAún no hay calificaciones
- Religiosity Prevalence and Its Association With Depression and Anxiety Symptoms Among Hispanic/Latino AdultsDocumento14 páginasReligiosity Prevalence and Its Association With Depression and Anxiety Symptoms Among Hispanic/Latino AdultsYenny Johanna Baron LondoñoAún no hay calificaciones
- Children: Social Determinants of Perceived Discrimination Among Black Youth: Intersection of Ethnicity and GenderDocumento11 páginasChildren: Social Determinants of Perceived Discrimination Among Black Youth: Intersection of Ethnicity and GenderAnthropophobe NyctophileAún no hay calificaciones
- Psychosocial Aspects of Mexican-American, and Black Teenage PregnancyDocumento6 páginasPsychosocial Aspects of Mexican-American, and Black Teenage PregnancyMuhammad Avicenna Abdul SyukurAún no hay calificaciones
- Violencia ParejaDocumento8 páginasViolencia ParejaLaloAún no hay calificaciones
- Mental Health and Social Characteristic of HomelessDocumento7 páginasMental Health and Social Characteristic of HomelessCesar OstolazaAún no hay calificaciones
- Encuesta AdolescentesDocumento10 páginasEncuesta AdolescentesAdolfoLaraRdzAún no hay calificaciones
- Pi Is 0890856713004796Documento15 páginasPi Is 0890856713004796adrianaAún no hay calificaciones
- What I Have LearnedDocumento14 páginasWhat I Have LearnedALLAN JUNTILLAún no hay calificaciones
- Annotated Bibliography On Poverty in The United StatesDocumento5 páginasAnnotated Bibliography On Poverty in The United Statesapi-318406991Aún no hay calificaciones
- Redefining Trauma - Utilizing Restorative Justice To Repair Care SDocumento53 páginasRedefining Trauma - Utilizing Restorative Justice To Repair Care SLacatus OlimpiuAún no hay calificaciones
- Alexa RamirezDocumento8 páginasAlexa Ramirezapi-406809806Aún no hay calificaciones
- Equidad de Genero en El AccesoDocumento18 páginasEquidad de Genero en El AccesoAlejandra BeecheAún no hay calificaciones
- Body Image in Hispanic-Latino vs. European American AdolescentsDocumento17 páginasBody Image in Hispanic-Latino vs. European American AdolescentsDesiré Abrante RodríguezAún no hay calificaciones
- Hispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research Literature Prepared by Luis H. Zayas, Ph.D.Documento2 páginasHispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research Literature Prepared by Luis H. Zayas, Ph.D.UrbanYouthJusticeAún no hay calificaciones
- Child Cohort StudiesDocumento13 páginasChild Cohort Studiesk_dias6701Aún no hay calificaciones
- FM MammographyDocumento5 páginasFM MammographyAdita DitaAún no hay calificaciones
- Research Paper On Aids in AmericaDocumento6 páginasResearch Paper On Aids in Americajssoulznd100% (1)
- SexualidadDocumento22 páginasSexualidadVIOLETA HERMOZA CARDENASAún no hay calificaciones
- Injustice Latino English VersionDocumento4 páginasInjustice Latino English VersionBenny CartwrightAún no hay calificaciones
- Psychotropic Medication Nonadherence Among United States Latinos: A Comprehensive Literature ReviewDocumento19 páginasPsychotropic Medication Nonadherence Among United States Latinos: A Comprehensive Literature ReviewpoopmanAún no hay calificaciones
- MM 24Documento32 páginasMM 24worksheetbookAún no hay calificaciones
- HMP 601 Midterm PaperDocumento4 páginasHMP 601 Midterm PaperDavontae Foxx-DrewAún no hay calificaciones
- Stephenson2007 PDFDocumento13 páginasStephenson2007 PDFLuis AlvaradoAún no hay calificaciones
- ERQ AcculturationDocumento2 páginasERQ AcculturationCharlesAún no hay calificaciones
- Women of Color 2006Documento194 páginasWomen of Color 2006mohanvelin100% (1)
- Incidence of Diabetes in Youth in The United States: Original ContributionDocumento10 páginasIncidence of Diabetes in Youth in The United States: Original ContributionAnnisa FujiantiAún no hay calificaciones
- Sexually Transmitted Infection Prevention Project As Community-Engaged ScholarshipDocumento9 páginasSexually Transmitted Infection Prevention Project As Community-Engaged Scholarshipnek ocinrocAún no hay calificaciones
- Health Insurance and Access To Care For Families With Young Children in CaliforniaDocumento9 páginasHealth Insurance and Access To Care For Families With Young Children in CaliforniaarisuimasuAún no hay calificaciones
- PYROOZ e SWEETEN - Gang Membership Between Ages 5 and 17 Years in The United StatesDocumento6 páginasPYROOZ e SWEETEN - Gang Membership Between Ages 5 and 17 Years in The United StatesEduardo Matos de AlencarAún no hay calificaciones
- Research Article: Factors Associated With Anxiety and Depression Among African American and White WomenDocumento9 páginasResearch Article: Factors Associated With Anxiety and Depression Among African American and White WomenMa. Angela CastronuevoAún no hay calificaciones
- 1 s2.0 0160798781900338 MainDocumento8 páginas1 s2.0 0160798781900338 MainParis Oliver González RuizAún no hay calificaciones
- Karlsen Nazroo 2011 Relation Between Racial Discrimination Social Class and Health Among Ethnic Minority GroupsDocumento8 páginasKarlsen Nazroo 2011 Relation Between Racial Discrimination Social Class and Health Among Ethnic Minority GroupslunamadalengoitiafrancoAún no hay calificaciones
- Vicente Child PDFDocumento11 páginasVicente Child PDFEduardo GonzálezAún no hay calificaciones
- Lorayna Lucero Literature ReviewDocumento8 páginasLorayna Lucero Literature Reviewapi-625810912Aún no hay calificaciones
- Barrett Impulsiveness Scale (BIS-11)Documento10 páginasBarrett Impulsiveness Scale (BIS-11)andr3yl0Aún no hay calificaciones
- Survey of Mexican Migrants: The Economic Transition To AmericaDocumento42 páginasSurvey of Mexican Migrants: The Economic Transition To AmericancmodularAún no hay calificaciones
- Long-Term Consequences of Childhood Sexual Abuse by Gender of VictimDocumento9 páginasLong-Term Consequences of Childhood Sexual Abuse by Gender of VictimMalyasree BasuAún no hay calificaciones
- CHSI - SequatchieDocumento8 páginasCHSI - SequatchieerlangerhealthAún no hay calificaciones
- Health Care and Education Access of Transnational Children in MexDocumento49 páginasHealth Care and Education Access of Transnational Children in MexLatinos Ready To VoteAún no hay calificaciones
- Acute Kidney Injury: Chapter ContentsDocumento22 páginasAcute Kidney Injury: Chapter ContentsnasimhsAún no hay calificaciones
- Acute Kidney Injury: Mark BevanDocumento42 páginasAcute Kidney Injury: Mark BevannasimhsAún no hay calificaciones
- Accelerated Idioventricular RhythmDocumento4 páginasAccelerated Idioventricular RhythmnasimhsAún no hay calificaciones
- Performing An A-G Patient Assessment: A Step-By-Step GuideDocumento3 páginasPerforming An A-G Patient Assessment: A Step-By-Step GuidenasimhsAún no hay calificaciones
- Acute Decompensated Heart Failure: A Study of Nursing CareDocumento12 páginasAcute Decompensated Heart Failure: A Study of Nursing CarenasimhsAún no hay calificaciones
- Using A Systematic Approach To Assess An Acutely Unwell Patient With Catatonia: A Case StudyDocumento9 páginasUsing A Systematic Approach To Assess An Acutely Unwell Patient With Catatonia: A Case StudynasimhsAún no hay calificaciones
- Job Description / Competency Profile: Job Title Payband/Grade Directorate Job Description ReferenceDocumento5 páginasJob Description / Competency Profile: Job Title Payband/Grade Directorate Job Description ReferencenasimhsAún no hay calificaciones
- PT - and NursesDocumento7 páginasPT - and NursesnasimhsAún no hay calificaciones
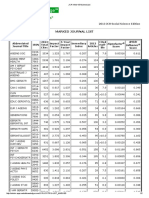
- Marked Journal List: 2013 JCR Social Science EditionDocumento2 páginasMarked Journal List: 2013 JCR Social Science EditionnasimhsAún no hay calificaciones
- 14.4 MSDocumento14 páginas14.4 MSnasimhsAún no hay calificaciones
- Marked Journal List: 2013 JCR Social Science EditionDocumento2 páginasMarked Journal List: 2013 JCR Social Science EditionnasimhsAún no hay calificaciones
- Marked Journal List: 2013 JCR Social Science EditionDocumento2 páginasMarked Journal List: 2013 JCR Social Science EditionnasimhsAún no hay calificaciones
- Marked Journal List: 2013 JCR Social Science EditionDocumento2 páginasMarked Journal List: 2013 JCR Social Science EditionnasimhsAún no hay calificaciones
- Accelerated Idioventricular RhythmDocumento4 páginasAccelerated Idioventricular RhythmnasimhsAún no hay calificaciones
- Nclex Lab ValuesDocumento6 páginasNclex Lab ValuesnasimhsAún no hay calificaciones
- Which of The Following Statements About The Human Nervous System Is True?Documento12 páginasWhich of The Following Statements About The Human Nervous System Is True?nasimhsAún no hay calificaciones
- (IELTSMaterial - Com) 100 IELTS Speaking Part 2 Topics in 2016 & 2017 & Sample Answers PDFDocumento135 páginas(IELTSMaterial - Com) 100 IELTS Speaking Part 2 Topics in 2016 & 2017 & Sample Answers PDFUyenAún no hay calificaciones
- AirwayDocumento2 páginasAirwaynasimhsAún no hay calificaciones
- Blood TubesDocumento1 páginaBlood TubesnasimhsAún no hay calificaciones
- Media PDFDocumento21 páginasMedia PDFlethuhaiAún no hay calificaciones
- Role of Observational Medicine in EmergencyDocumento13 páginasRole of Observational Medicine in EmergencyazhaabazAún no hay calificaciones
- Lex-Mental HealthDocumento49 páginasLex-Mental HealthnasimhsAún no hay calificaciones
- Pharmacology Review For NursesDocumento11 páginasPharmacology Review For Nursesisabel_avancena100% (4)
- λεξ ψ υγειαDocumento87 páginasλεξ ψ υγειαnasimhsAún no hay calificaciones
- Weight Box SHOTDocumento1 páginaWeight Box SHOTnasimhsAún no hay calificaciones
- Nerve SynapseDocumento2 páginasNerve SynapsenasimhsAún no hay calificaciones
- OET Writing and Speaking Made Easy For NursesDocumento143 páginasOET Writing and Speaking Made Easy For NursesLiju K Oommen97% (33)
- Pharmacology Review For NursesDocumento11 páginasPharmacology Review For Nursesisabel_avancena100% (4)
- Unexpected Transfusion blc6991p FinalDocumento2 páginasUnexpected Transfusion blc6991p FinalnasimhsAún no hay calificaciones
- Common Laboratory Values PDF GreenDocumento11 páginasCommon Laboratory Values PDF GreennasimhsAún no hay calificaciones
- 40agilemethodsin40minutes 141020221938 Conversion Gate01 PDFDocumento104 páginas40agilemethodsin40minutes 141020221938 Conversion Gate01 PDFpjsystemAún no hay calificaciones
- Project ManagementDocumento34 páginasProject ManagementFarhan TariqAún no hay calificaciones
- Reproduced or Transmitted Without Publisher's Prior Permission. Violators Will Be ProsecutedDocumento10 páginasReproduced or Transmitted Without Publisher's Prior Permission. Violators Will Be Prosecutedbologaw846Aún no hay calificaciones
- Maclaurin 14Documento3 páginasMaclaurin 14ichkhuyAún no hay calificaciones
- Low-Permeability Concrete Water-To-Cement Ratio Optimization For Designing Drinking Water ReservoirsDocumento5 páginasLow-Permeability Concrete Water-To-Cement Ratio Optimization For Designing Drinking Water ReservoirsInternational Journal of Innovations in Engineering and ScienceAún no hay calificaciones
- General Biology 2 Midterms GRASPSDocumento2 páginasGeneral Biology 2 Midterms GRASPSAlbert RoseteAún no hay calificaciones
- Problem Sheet V - ANOVADocumento5 páginasProblem Sheet V - ANOVARuchiMuchhalaAún no hay calificaciones
- Data Mining in The Insurance Industry - Solving Business Problems Using SAS Enterprise Miner SoftwareDocumento20 páginasData Mining in The Insurance Industry - Solving Business Problems Using SAS Enterprise Miner SoftwareShehan1Aún no hay calificaciones
- Kurt LewinDocumento8 páginasKurt Lewinmaria_bianco679079Aún no hay calificaciones
- Kimia Percubaan SPM 2009 Kertas 1, 2, 3 MRSMDocumento68 páginasKimia Percubaan SPM 2009 Kertas 1, 2, 3 MRSMCarolyn Chang Boon ChuiAún no hay calificaciones
- New Curriculum of Class 11 and 12 Optional Subject First 2076Documento157 páginasNew Curriculum of Class 11 and 12 Optional Subject First 2076Narendra KhadkaAún no hay calificaciones
- TrainingGuide Geomatica 1 2017Documento132 páginasTrainingGuide Geomatica 1 2017sam.scribdAún no hay calificaciones
- Finding Herself. KelloggDocumento12 páginasFinding Herself. KelloggMinerva MinasAún no hay calificaciones
- Using Keyframe SynfigDocumento1 páginaUsing Keyframe SynfigNdandungAún no hay calificaciones
- HRM ThreeshortcasesDocumento4 páginasHRM ThreeshortcaseskhanmohsinjamilAún no hay calificaciones
- ERPDocumento9 páginasERPWindadahri PuslitkaretAún no hay calificaciones
- 749481Documento3 páginas749481PAULSON K ANTONY 17BEC1147100% (1)
- Rapport - FEEDBACK INFRA - ODIENNE - V01 - ANGLAISDocumento25 páginasRapport - FEEDBACK INFRA - ODIENNE - V01 - ANGLAISabertoAún no hay calificaciones
- Solar TimeDocumento3 páginasSolar TimeAkshay Deshpande0% (1)
- The Use of Electrical Resistivity Tomography (ERT) To Delineate W PDFDocumento76 páginasThe Use of Electrical Resistivity Tomography (ERT) To Delineate W PDFConstantin UngureanuAún no hay calificaciones
- Sample Codal ComplianceDocumento1 páginaSample Codal Complianceshangz1511Aún no hay calificaciones
- Web Security Unit 6 Notes PDFDocumento24 páginasWeb Security Unit 6 Notes PDFMohd FareeduddinAún no hay calificaciones
- Team Meeting - 6th MayDocumento11 páginasTeam Meeting - 6th MaySachin SharmaAún no hay calificaciones
- Industrial PsychologyDocumento4 páginasIndustrial PsychologyNeo VeloriaAún no hay calificaciones
- Maths InterviewDocumento6 páginasMaths InterviewKeamogetse BoitshwareloAún no hay calificaciones
- How To Modify Standard PF-Status of ALV GridDocumento4 páginasHow To Modify Standard PF-Status of ALV GridAshish MohapatraAún no hay calificaciones
- Monograph 33Documento106 páginasMonograph 33Karthik Abhi100% (1)
- Yameena Rashid: ObjectivesDocumento2 páginasYameena Rashid: ObjectivesMisbhasaeedaAún no hay calificaciones
- Cenizas de Izalco - Capitulos 1 Al 15Documento26 páginasCenizas de Izalco - Capitulos 1 Al 15Gafriel100% (3)
- Classified2018 10 15586115Documento7 páginasClassified2018 10 15586115janoosAún no hay calificaciones
- Summary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesDe EverandSummary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesCalificación: 5 de 5 estrellas5/5 (1635)
- The Power of Now: A Guide to Spiritual EnlightenmentDe EverandThe Power of Now: A Guide to Spiritual EnlightenmentCalificación: 4.5 de 5 estrellas4.5/5 (4125)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionCalificación: 4 de 5 estrellas4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityCalificación: 4 de 5 estrellas4/5 (26)
- The Stoic Mindset: Living the Ten Principles of StoicismDe EverandThe Stoic Mindset: Living the Ten Principles of StoicismCalificación: 5 de 5 estrellas5/5 (7)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsCalificación: 5 de 5 estrellas5/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedCalificación: 5 de 5 estrellas5/5 (81)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeCalificación: 2 de 5 estrellas2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAún no hay calificaciones
- Becoming Supernatural: How Common People Are Doing The UncommonDe EverandBecoming Supernatural: How Common People Are Doing The UncommonCalificación: 5 de 5 estrellas5/5 (1480)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Calificación: 4.5 de 5 estrellas4.5/5 (110)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDCalificación: 5 de 5 estrellas5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Silva Mind Method: for Getting Help from the Other SideDe EverandThe Silva Mind Method: for Getting Help from the Other SideCalificación: 5 de 5 estrellas5/5 (51)
- Indistractable: How to Control Your Attention and Choose Your LifeDe EverandIndistractable: How to Control Your Attention and Choose Your LifeCalificación: 3 de 5 estrellas3/5 (5)
- Master Your Emotions: Develop Emotional Intelligence and Discover the Essential Rules of When and How to Control Your FeelingsDe EverandMaster Your Emotions: Develop Emotional Intelligence and Discover the Essential Rules of When and How to Control Your FeelingsCalificación: 4.5 de 5 estrellas4.5/5 (321)
- Summary: The Laws of Human Nature: by Robert Greene: Key Takeaways, Summary & AnalysisDe EverandSummary: The Laws of Human Nature: by Robert Greene: Key Takeaways, Summary & AnalysisCalificación: 4.5 de 5 estrellas4.5/5 (30)
- The 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageDe EverandThe 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageCalificación: 5 de 5 estrellas5/5 (73)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsCalificación: 4.5 de 5 estrellas4.5/5 (170)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsCalificación: 3.5 de 5 estrellas3.5/5 (3)
- The One Thing: The Surprisingly Simple Truth Behind Extraordinary ResultsDe EverandThe One Thing: The Surprisingly Simple Truth Behind Extraordinary ResultsCalificación: 4.5 de 5 estrellas4.5/5 (709)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityCalificación: 4 de 5 estrellas4/5 (3)
- Uptime: A Practical Guide to Personal Productivity and WellbeingDe EverandUptime: A Practical Guide to Personal Productivity and WellbeingAún no hay calificaciones
- The Science of Self Discipline: How Daily Self-Discipline, Everyday Habits and an Optimised Belief System will Help You Beat Procrastination + Why Discipline Equals True FreedomDe EverandThe Science of Self Discipline: How Daily Self-Discipline, Everyday Habits and an Optimised Belief System will Help You Beat Procrastination + Why Discipline Equals True FreedomCalificación: 4.5 de 5 estrellas4.5/5 (867)