También podría gustarte
- The Critical Care Management of Poor SAHDocumento19 páginasThe Critical Care Management of Poor SAHBeny RiliantoAún no hay calificaciones
- Osmotic Demyelination Syndrome.Documento5 páginasOsmotic Demyelination Syndrome.Nontaphon PiyawattanamethaAún no hay calificaciones
- Post Traumatic SyringomyeliaDocumento7 páginasPost Traumatic SyringomyeliaNontaphon PiyawattanamethaAún no hay calificaciones
- Cryopreservation Versus Subcutaneous Preservation of Autologous Bone Flaps For CranioplastyDocumento5 páginasCryopreservation Versus Subcutaneous Preservation of Autologous Bone Flaps For CranioplastyNontaphon PiyawattanamethaAún no hay calificaciones
- Cerebrospinal Fluid Diversion in A Myelomeningocele PopulationDocumento6 páginasCerebrospinal Fluid Diversion in A Myelomeningocele PopulationNontaphon PiyawattanamethaAún no hay calificaciones
- ICD-9-CM 2015 Professional Edition For Hospitals, Vols 1, 2 and 3 (AMA) (PDF) (UnitedVRG)Documento1330 páginasICD-9-CM 2015 Professional Edition For Hospitals, Vols 1, 2 and 3 (AMA) (PDF) (UnitedVRG)Nontaphon PiyawattanamethaAún no hay calificaciones
- Pain PerceptionDocumento3 páginasPain PerceptionNontaphon PiyawattanamethaAún no hay calificaciones
- Low-Dose Aspirin in The Primary Prevention of Cardiovascular DiseaseDocumento2 páginasLow-Dose Aspirin in The Primary Prevention of Cardiovascular DiseaseNontaphon PiyawattanamethaAún no hay calificaciones
- Steroid For ASIDocumento54 páginasSteroid For ASINontaphon PiyawattanamethaAún no hay calificaciones
- Aspirin For Primary Prevention of Atherosclerotic Cardiovascular Disease PDFDocumento10 páginasAspirin For Primary Prevention of Atherosclerotic Cardiovascular Disease PDFNontaphon PiyawattanamethaAún no hay calificaciones
- Cryopreservation Versus Subcutaneous Preservation of Autologous Bone Flaps For CranioplastyDocumento5 páginasCryopreservation Versus Subcutaneous Preservation of Autologous Bone Flaps For CranioplastyNontaphon PiyawattanamethaAún no hay calificaciones
- Treatment Recurrence HCC After LTDocumento42 páginasTreatment Recurrence HCC After LTNontaphon PiyawattanamethaAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (120)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2101)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- An Uncommon CourtshipDocumento32 páginasAn Uncommon CourtshipBethany House PublishersAún no hay calificaciones
- OsteomyelitisDocumento15 páginasOsteomyelitisJayvee Ampo100% (2)
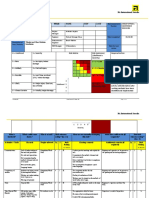
- Standard RA Template-1Documento3 páginasStandard RA Template-1Bhuvanesh SriniAún no hay calificaciones
- Clinical SciencesDocumento6 páginasClinical Sciencesapi-301251642Aún no hay calificaciones
- Anatomy Notes For BS: Khyber Medical University Peshawar Prepared by DR, Raheel Ahmad Lecturer Pihms. PeshawarDocumento84 páginasAnatomy Notes For BS: Khyber Medical University Peshawar Prepared by DR, Raheel Ahmad Lecturer Pihms. PeshawarShimmering MoonAún no hay calificaciones
- Investigation of An Animal Mutilation Injuries in Cache County, UtahDocumento33 páginasInvestigation of An Animal Mutilation Injuries in Cache County, UtahLionel Elyansun100% (1)
- Etkb Bonus A PDFDocumento23 páginasEtkb Bonus A PDFJacob Stone100% (2)
- BandagingDocumento12 páginasBandagingJUANJOSEFOXAún no hay calificaciones
- Science6 Q2 Mod1 TheHumanBodySystems V4Documento30 páginasScience6 Q2 Mod1 TheHumanBodySystems V4ThievesPHAún no hay calificaciones
- Achilles Tendon RuptureDocumento3 páginasAchilles Tendon RuptureAntonius ElawitachyaAún no hay calificaciones
- Tuesday, 11 April 2017 14:14: Primer On The April 2017 Series of Earthquakes in Batangas ProvinceDocumento7 páginasTuesday, 11 April 2017 14:14: Primer On The April 2017 Series of Earthquakes in Batangas ProvinceJamaica RamosAún no hay calificaciones
- Seidel's TestDocumento13 páginasSeidel's TestFahcrezaAún no hay calificaciones
- Injury Report 2011Documento20 páginasInjury Report 2011Andrea ContiAún no hay calificaciones
- K1 - Initial AssessmentDocumento34 páginasK1 - Initial Assessmentpuja argaAún no hay calificaciones
- Legal and TaxDocumento35 páginasLegal and TaxSachin MethreeAún no hay calificaciones
- Wrist Anatomy and Surgical Approaches: Roy Cardoso, MD, Robert M. Szabo, MD, MPHDocumento22 páginasWrist Anatomy and Surgical Approaches: Roy Cardoso, MD, Robert M. Szabo, MD, MPHMd Ahsanuzzaman PinkuAún no hay calificaciones
- AGUADO - Diseño de Órtesis en Impresión 3D PDFDocumento84 páginasAGUADO - Diseño de Órtesis en Impresión 3D PDFJoel Kevin GonzalesAún no hay calificaciones
- Indicadores ICMM PDFDocumento16 páginasIndicadores ICMM PDFJesús Omar Solís100% (1)
- Biomechanics of The Knee 1Documento2 páginasBiomechanics of The Knee 1savitha sabuAún no hay calificaciones
- Plex Nonskeletal Problems in Preadolescent ChildrenDocumento5 páginasPlex Nonskeletal Problems in Preadolescent ChildrenyasmineAún no hay calificaciones
- Angle Grinder PDFDocumento2 páginasAngle Grinder PDFcityofdarwingisAún no hay calificaciones
- Ekonomski Uticaj Saobracajnih NezgodaDocumento304 páginasEkonomski Uticaj Saobracajnih NezgodaJablan M KaraklajicAún no hay calificaciones
- Fluid Management in Neurology & Neurocritical Care: DR Nagesh JadavDocumento12 páginasFluid Management in Neurology & Neurocritical Care: DR Nagesh JadavNagesh JadavAún no hay calificaciones
- Risk Assessment - Window and Glass Partition InstallationDocumento4 páginasRisk Assessment - Window and Glass Partition Installationburak80% (5)
- AphasiaDocumento35 páginasAphasiadikri pangersa100% (2)
- Clinical Preview About Hernia: It's Types, Clinical Presentation, Diagnosis and RepairDocumento10 páginasClinical Preview About Hernia: It's Types, Clinical Presentation, Diagnosis and RepairAfnan AdelAún no hay calificaciones
- Hip Muscle Activity During Isometric Contraction of Hip AbductionDocumento4 páginasHip Muscle Activity During Isometric Contraction of Hip AbductionDaniel FreireAún no hay calificaciones
- Doppler Ultrasonography of Lower Extremity ArterieDocumento35 páginasDoppler Ultrasonography of Lower Extremity Arterierizki100% (1)
- The Verdict 1982 PDFDocumento126 páginasThe Verdict 1982 PDFNick LaurAún no hay calificaciones
- The Slave and The Lion: (Time - 3.18)Documento1 páginaThe Slave and The Lion: (Time - 3.18)Mohammad AwaisAún no hay calificaciones