También podría gustarte
- Medicolegal Death Investigation: A Step-By-Step Field GuideDe EverandMedicolegal Death Investigation: A Step-By-Step Field GuideAún no hay calificaciones
- Blue FormDocumento2 páginasBlue Formalin_capilnean8371Aún no hay calificaciones
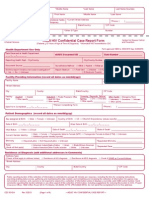
- Adult HIV Confidential Case Report FormDocumento4 páginasAdult HIV Confidential Case Report FormilyaskureshiAún no hay calificaciones
- Format for Recording Medical ExamsDocumento4 páginasFormat for Recording Medical ExamsDany David-Diculescu56% (9)
- Medical Records SummaryDocumento2 páginasMedical Records SummarynjunaidiAún no hay calificaciones
- Admission and DischargeDocumento4 páginasAdmission and DischargeTribhuwan KushwahaAún no hay calificaciones
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocumento5 páginasKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiAún no hay calificaciones
- Guidelines To Fill in Health Examination ReportDocumento6 páginasGuidelines To Fill in Health Examination ReportNurman HidayatAún no hay calificaciones
- Form G Health Examination Report International StudentDocumento6 páginasForm G Health Examination Report International StudentVictor OjukwuAún no hay calificaciones
- Incident Report Form: Docx Duworks EsourcesDocumento1 páginaIncident Report Form: Docx Duworks EsourcesKrishma PanjetaAún no hay calificaciones
- Home Protector ApplicationDocumento5 páginasHome Protector ApplicationDejanAún no hay calificaciones
- Report a Workplace InjuryDocumento1 páginaReport a Workplace InjuryHema PriyaAún no hay calificaciones
- The WHO 2016 International Medical Certificate of Cause of Death FormDocumento4 páginasThe WHO 2016 International Medical Certificate of Cause of Death FormFira GorjessAún no hay calificaciones
- Form No.4 (See Rule 7) Medical Certificate of Cause of DeathDocumento4 páginasForm No.4 (See Rule 7) Medical Certificate of Cause of DeathBeyza GemiciAún no hay calificaciones
- D ReportDocumento2 páginasD ReportHihiAún no hay calificaciones
- Personal Accident'S / Accident Medical Reimbursement'S Attending Physician'S StatementDocumento4 páginasPersonal Accident'S / Accident Medical Reimbursement'S Attending Physician'S Statementts8166Aún no hay calificaciones
- Certification of Cause of DeathDocumento9 páginasCertification of Cause of DeathMoses MwauraAún no hay calificaciones
- Death CertificateDocumento3 páginasDeath CertificateAllen Peter WeixlerAún no hay calificaciones
- C105a Pre-Sea and Periodic Medical Fitness Examinations For SeafarersDocumento4 páginasC105a Pre-Sea and Periodic Medical Fitness Examinations For SeafarersAbu ShabeelAún no hay calificaciones
- Galveston Orientation Amnesia TestDocumento1 páginaGalveston Orientation Amnesia TestCaliph IVAún no hay calificaciones
- Report of Medical History: PhoneDocumento3 páginasReport of Medical History: PhoneLeroy Jethro Gibbs NicosiaAún no hay calificaciones
- People of The PhilippinesDocumento6 páginasPeople of The PhilippinesNyx PerezAún no hay calificaciones
- Cs Form 100 Rev Nov 2012Documento2 páginasCs Form 100 Rev Nov 2012Amanda PattersonAún no hay calificaciones
- Complete The Following Paragraph With The Most Suitable Words From The Box. (Almost Words Are Used Once Only and Some Others Are Not Used)Documento5 páginasComplete The Following Paragraph With The Most Suitable Words From The Box. (Almost Words Are Used Once Only and Some Others Are Not Used)Mỹ Ngọc Trâm LêAún no hay calificaciones
- Student Health Form - FinalDocumento3 páginasStudent Health Form - Finalbrown_chocolate87643Aún no hay calificaciones
- Cause of Death Quick Fact SheetDocumento2 páginasCause of Death Quick Fact SheettrialqwAún no hay calificaciones
- MSK Cancer Center CV & Bibliography GuideDocumento5 páginasMSK Cancer Center CV & Bibliography GuidePia AAún no hay calificaciones
- Doctor's Name, Surname or Name of Hospital/Health CenterDocumento2 páginasDoctor's Name, Surname or Name of Hospital/Health CenterFika JeAún no hay calificaciones
- TBJ New Patient Registration FormsDocumento9 páginasTBJ New Patient Registration FormsSandra RíosAún no hay calificaciones
- Linda Winters - Victim Impact StatementDocumento6 páginasLinda Winters - Victim Impact StatementOmar Ha-RedeyeAún no hay calificaciones
- Memorial Sloan Kettering Cancer Center Curriculum Vitae and BibliographyDocumento6 páginasMemorial Sloan Kettering Cancer Center Curriculum Vitae and BibliographyOncoshravanAún no hay calificaciones
- HKCAD Medical Report FormDocumento4 páginasHKCAD Medical Report FormHelloWorldAún no hay calificaciones
- REGISTRATION DOCUMENT APPENDICESDocumento14 páginasREGISTRATION DOCUMENT APPENDICESHariBoy NotSo FreeTodayAún no hay calificaciones
- Instructions For Leishmanises Register: Day / Month / Year (DD/MM/YY) (EC)Documento2 páginasInstructions For Leishmanises Register: Day / Month / Year (DD/MM/YY) (EC)Dagnachew MulugetaAún no hay calificaciones
- Form PD1 Medical Examination ReportDocumento9 páginasForm PD1 Medical Examination ReportSyazwi BaharuddinAún no hay calificaciones
- 2008 NYState Annual AIDSSurveillance ReportDocumento90 páginas2008 NYState Annual AIDSSurveillance ReporthousingworksAún no hay calificaciones
- Date Medical History Taken: - / - /20Documento7 páginasDate Medical History Taken: - / - /20Glogogeanu Cristina AndreeaAún no hay calificaciones
- OSCE/OSPE EXAM GUIDEDocumento51 páginasOSCE/OSPE EXAM GUIDELouise Tan100% (3)
- Medical Certificate ProformaDocumento2 páginasMedical Certificate ProformaAnulal .sAún no hay calificaciones
- Form 4ADocumento2 páginasForm 4Adr.bhadarkaAún no hay calificaciones
- Targeted Patient Safety QuestionnairesDocumento27 páginasTargeted Patient Safety QuestionnairesAafreen KhairAún no hay calificaciones
- PDSDocumento4 páginasPDSMariele Tokong Montederamos-ConteAún no hay calificaciones
- Notes On How To Fill in The Medical Certificate of Cause of DeathDocumento10 páginasNotes On How To Fill in The Medical Certificate of Cause of DeathSayantan BanerjeeAún no hay calificaciones
- DD2808Report of Medical ExaminationDocumento3 páginasDD2808Report of Medical Examinationk_tanjaAún no hay calificaciones
- Incident ReportDocumento3 páginasIncident Reportthuynh12Aún no hay calificaciones
- Medical Certificate of Cause of DeathDocumento12 páginasMedical Certificate of Cause of DeathTara WandhitaAún no hay calificaciones
- Personal Data Sheet: 1. CS ID No. I. Personal InformationDocumento4 páginasPersonal Data Sheet: 1. CS ID No. I. Personal InformationSachi SummersAún no hay calificaciones
- Ihsaa Pre-Participation Physical Evaluation: School: HistoryDocumento4 páginasIhsaa Pre-Participation Physical Evaluation: School: HistoryLinden Seitz100% (1)
- Civil Service Exam Application Form GuideDocumento2 páginasCivil Service Exam Application Form GuideAnnAún no hay calificaciones
- UK Death Certificate OSCE GuideDocumento6 páginasUK Death Certificate OSCE GuideAdil IslamAún no hay calificaciones
- Appendix F: Suggested Format For Recording Medical Examinations of SeafarersDocumento5 páginasAppendix F: Suggested Format For Recording Medical Examinations of SeafarersGabrielAún no hay calificaciones
- Patient Summary FormDocumento1 páginaPatient Summary FormPopeJr Greyhound-BaseballAún no hay calificaciones
- SRF ICMR Kerala - PDF (New) PDFDocumento2 páginasSRF ICMR Kerala - PDF (New) PDFRenjithAún no hay calificaciones
- Um Health Examination Form New 2016Documento6 páginasUm Health Examination Form New 2016Saoirse MinAún no hay calificaciones
- Hospital StandardQC FormsDocumento22 páginasHospital StandardQC FormstotqmAún no hay calificaciones
- PDS (Revised 2005)Documento4 páginasPDS (Revised 2005)Pulisya Ng Sta Ana100% (1)
- Undergraduate Application FormDocumento5 páginasUndergraduate Application Formpsiziba6702100% (1)
- INSTRUCTIONS: DD Form 1380, Tactical Combat Casualty Care (TCCC) Card (Formerly: U.S. Field Medical Card) 1. Background and PurposeDocumento2 páginasINSTRUCTIONS: DD Form 1380, Tactical Combat Casualty Care (TCCC) Card (Formerly: U.S. Field Medical Card) 1. Background and Purposednzcarboni1Aún no hay calificaciones
- PDS - PinayDocumento4 páginasPDS - PinayFridilyn AlconesAún no hay calificaciones
- Sbar Report Cue Sheet Oct 18Documento2 páginasSbar Report Cue Sheet Oct 18haaris 7khanAún no hay calificaciones
- Health Assessment Final ReviewerDocumento40 páginasHealth Assessment Final ReviewerlumpiaAún no hay calificaciones
- International Journal of Trend in Scientific Research and Development (IJTSRD)Documento31 páginasInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDAún no hay calificaciones
- Heart Failure - A Clinical Nursing HandbookDocumento273 páginasHeart Failure - A Clinical Nursing Handbookjustbeingclever100% (2)
- Physiological Changes During Pregnancy 2010Documento42 páginasPhysiological Changes During Pregnancy 2010Asyhok Renault100% (1)
- BPEd Syllabus UpdateDocumento101 páginasBPEd Syllabus UpdateNaga DAún no hay calificaciones
- SVT PresentationDocumento39 páginasSVT PresentationReinsy NoviAún no hay calificaciones
- Effects of Stun Guns and TasersDocumento2 páginasEffects of Stun Guns and TasersRed PhoenixAún no hay calificaciones
- BIO 202 Circulation I Lab 22S PDFDocumento2 páginasBIO 202 Circulation I Lab 22S PDFTraci GardnerAún no hay calificaciones
- Case StudyDocumento7 páginasCase StudyBiway RegalaAún no hay calificaciones
- IV. Antiarrhythmic Drugs: PHRM 537 Summer 2020Documento19 páginasIV. Antiarrhythmic Drugs: PHRM 537 Summer 2020SaulAún no hay calificaciones
- Module in Science DoneeeeeDocumento35 páginasModule in Science DoneeeeeManelyn TagaAún no hay calificaciones
- Rsud Pasar Rebo Intensive Coronary Care Unit/Iccu Rsud Pasar Rebo Intensive Coronary Care Unit/IccuDocumento5 páginasRsud Pasar Rebo Intensive Coronary Care Unit/Iccu Rsud Pasar Rebo Intensive Coronary Care Unit/IccurizasatryaAún no hay calificaciones
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocumento1 páginaAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalAún no hay calificaciones
- MD Development PaediatrcsDocumento102 páginasMD Development PaediatrcsMuhammad Farooq SaeedAún no hay calificaciones
- Physical Assessment of 11-Year-Old MaleDocumento12 páginasPhysical Assessment of 11-Year-Old MaleNoeclaire Jamandre TulodAún no hay calificaciones
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDocumento3 páginasDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)
- 9th Grade Science Lesson on the Cardiovascular SystemDocumento5 páginas9th Grade Science Lesson on the Cardiovascular SystemOliver VillanuevaAún no hay calificaciones
- MCQ Answer KeyDocumento46 páginasMCQ Answer KeyDr. RamadanAún no hay calificaciones
- The Anatomy and Functions of the Heart in 40 CharactersDocumento7 páginasThe Anatomy and Functions of the Heart in 40 CharactersMarjorie ViescaAún no hay calificaciones
- Psycopharmacology For PhysicianDocumento2 páginasPsycopharmacology For PhysicianSyawal PratamaAún no hay calificaciones
- Heart Health GuideDocumento7 páginasHeart Health GuideYAO CESAR KOFFIAún no hay calificaciones
- EkgppDocumento93 páginasEkgppLindsay WishmierAún no hay calificaciones
- Pulmonary EdemaDocumento2 páginasPulmonary EdemaMuhammad Bayu Zohari HutagalungAún no hay calificaciones
- FundamentalsDocumento30 páginasFundamentalsRachel PerandoAún no hay calificaciones
- Teleflex Interventional Ordering Catalog: Corporate OfficeDocumento50 páginasTeleflex Interventional Ordering Catalog: Corporate OfficeMuhammad Mahbøøb SadiqAún no hay calificaciones
- 8std Bio Ch-684981Documento6 páginas8std Bio Ch-684981Beast X GamingAún no hay calificaciones
- SDTM TerminologyDocumento512 páginasSDTM TerminologySuri VijayAún no hay calificaciones
- BME 461 ManualDocumento143 páginasBME 461 ManualMohmmad P.AlshormanAún no hay calificaciones
- Cardiomyopathy: Restrictive Heart DiseaseDocumento18 páginasCardiomyopathy: Restrictive Heart DiseaseMitch GabuyaAún no hay calificaciones
- The Six Second ECGDocumento6 páginasThe Six Second ECGRaquel GirónAún no hay calificaciones