También podría gustarte
- Development and Pilot Study of Group-Based Dietary Self-Management Program For Community Dwellers With HypertensionDocumento14 páginasDevelopment and Pilot Study of Group-Based Dietary Self-Management Program For Community Dwellers With HypertensionNur Fadillah B21741419601Aún no hay calificaciones
- Chronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldDocumento7 páginasChronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldHaneenAún no hay calificaciones
- Anderson 2009Documento18 páginasAnderson 2009Noviani RestaAún no hay calificaciones
- Healthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009De EverandHealthy Babies Are Worth The Wait: A Partnership to Reduce Preterm Births in Kentucky through Community-based Interventions 2007 - 2009Aún no hay calificaciones
- Cyt 113Documento12 páginasCyt 113Luis SolerAún no hay calificaciones
- Innes - Evaluacion DiferenciasDocumento10 páginasInnes - Evaluacion DiferenciasMaritzaAún no hay calificaciones
- 2019 Article 1059Documento12 páginas2019 Article 1059ρανιαAún no hay calificaciones
- Increasing Evidence-Based Workplace Health Promotion 2012Documento9 páginasIncreasing Evidence-Based Workplace Health Promotion 2012Frangolho JoãoAún no hay calificaciones
- Literature Review Dietary Services HospitalDocumento9 páginasLiterature Review Dietary Services Hospitalaflsrxfoe100% (1)
- Ramseier Et Al-2015-Journal of Clinical Periodontology PDFDocumento12 páginasRamseier Et Al-2015-Journal of Clinical Periodontology PDFChristine HacheAún no hay calificaciones
- Chronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldDocumento7 páginasChronic Illnesses Are Becoming An Increasingly Serious Public Health Issue Across The WorldHaneenAún no hay calificaciones
- The Science of Wellness Programs: A SynopsisDocumento53 páginasThe Science of Wellness Programs: A SynopsisPartnership to Fight Chronic Disease100% (1)
- Oti2018 7412686Documento17 páginasOti2018 7412686NataliaAún no hay calificaciones
- Select One of The Six Priority AreasDocumento3 páginasSelect One of The Six Priority AreasSadia SobanAún no hay calificaciones
- Food InterventionDocumento18 páginasFood InterventionAmani AlAún no hay calificaciones
- HGHJGVVVDocumento9 páginasHGHJGVVVMohamed SaudAún no hay calificaciones
- Conjoint in HEALTH ResearchDocumento17 páginasConjoint in HEALTH ResearchDiana Tan May KimAún no hay calificaciones
- WhoDocumento13 páginasWhoKCcheungAún no hay calificaciones
- Effect of Behavioral Weight Management Interventions Using Lifestyle Mhealth Self-Monitoring On Weight Loss A Systematic Review and Meta-AnalysisDocumento19 páginasEffect of Behavioral Weight Management Interventions Using Lifestyle Mhealth Self-Monitoring On Weight Loss A Systematic Review and Meta-Analysischieftains380Aún no hay calificaciones
- Nutritionatwork publishedOH2016Documento8 páginasNutritionatwork publishedOH2016chanisarembet25Aún no hay calificaciones
- Capturing Health and Eating Status Through A NutriDocumento13 páginasCapturing Health and Eating Status Through A NutriAniket VermaAún no hay calificaciones
- Ijerph 17 04664 v2Documento21 páginasIjerph 17 04664 v2vijay dagdiAún no hay calificaciones
- The Use of Smartphone Health Apps and Other Mobile Health (Mhealth) Technologies in Dietetic Practice - A Three Country StudyDocumento14 páginasThe Use of Smartphone Health Apps and Other Mobile Health (Mhealth) Technologies in Dietetic Practice - A Three Country StudyUmialqyAún no hay calificaciones
- 1471 2458 11 637Documento10 páginas1471 2458 11 637jlventiganAún no hay calificaciones
- Out 11Documento7 páginasOut 11AnamAún no hay calificaciones
- Using New Technologies To Promote Weight Management: A Randomised Controlled Trial Study ProtocolDocumento9 páginasUsing New Technologies To Promote Weight Management: A Randomised Controlled Trial Study Protocolasep9ustomAún no hay calificaciones
- 0rder 335 - Policy and Advocacy For Population HealthDocumento6 páginas0rder 335 - Policy and Advocacy For Population Healthjoshua chegeAún no hay calificaciones
- Nutrition and Physical Activity in Early Years Settings: A Qualitative Assessment of An Obesity Prevention ProgrammeDocumento5 páginasNutrition and Physical Activity in Early Years Settings: A Qualitative Assessment of An Obesity Prevention ProgrammegiaAún no hay calificaciones
- A Framework To Measure The Impact of Investments in Health ResearchDocumento16 páginasA Framework To Measure The Impact of Investments in Health ResearchGesler Pilvan SainAún no hay calificaciones
- n310 Health Promotion Research PaperDocumento7 páginasn310 Health Promotion Research Paperapi-239728993Aún no hay calificaciones
- Nutrients 07 05414 v3Documento12 páginasNutrients 07 05414 v3BernaluttaaaAún no hay calificaciones
- Evaluation of A Questionnaire To Assess Nutritional Knowledge, Attitudes and Practices in A Thai PopulationDocumento10 páginasEvaluation of A Questionnaire To Assess Nutritional Knowledge, Attitudes and Practices in A Thai PopulationUsman Ahmad TijjaniAún no hay calificaciones
- Group Interventions HealthDocumento10 páginasGroup Interventions HealthRosemary GonçalvesAún no hay calificaciones
- Spiby 2009Documento12 páginasSpiby 2009gabriela.grover.invest.nutAún no hay calificaciones
- Educational Training of Nutritionists inDocumento21 páginasEducational Training of Nutritionists inLarissa Araujo MaiaAún no hay calificaciones
- Public Health Nursing: Scope and Standards of PracticeDe EverandPublic Health Nursing: Scope and Standards of PracticeCalificación: 5 de 5 estrellas5/5 (1)
- Cabassa Et Al 2014Documento11 páginasCabassa Et Al 2014Eloisa Garcia AñinoAún no hay calificaciones
- Diet Optimization Using Linear ProgrammingDocumento8 páginasDiet Optimization Using Linear ProgrammingAnonymous vVsidh3nAún no hay calificaciones
- Qualitative PerspectivesDocumento8 páginasQualitative PerspectivesfiseradaAún no hay calificaciones
- 1471 2458 14 995 PDFDocumento10 páginas1471 2458 14 995 PDFSIRIUS RTAún no hay calificaciones
- Jurnas Bull2017Documento10 páginasJurnas Bull2017miftah zannahAún no hay calificaciones
- New Health Systems: Integrated Care and Health Inequalities ReductionDe EverandNew Health Systems: Integrated Care and Health Inequalities ReductionAún no hay calificaciones
- Agriculture, Food, and Nutrition Interventions That Facilitate Sustainable Food Production and Impact Health: An Overview of Systematic ReviewsDocumento9 páginasAgriculture, Food, and Nutrition Interventions That Facilitate Sustainable Food Production and Impact Health: An Overview of Systematic ReviewsAnonymous 6OPLC9UAún no hay calificaciones
- Perceptions, Attitudes, and Behaviors of Primary Care Providers Toward Obesity Management: A Qualitative StudyDocumento18 páginasPerceptions, Attitudes, and Behaviors of Primary Care Providers Toward Obesity Management: A Qualitative StudyFitriani WidyastantiAún no hay calificaciones
- Down 2020 5Documento16 páginasDown 2020 5Marie GuajardoAún no hay calificaciones
- WomenDocumento3 páginasWomenamarkumar42012Aún no hay calificaciones
- Food Labelling and Dietary Behaviour Bridging TheDocumento3 páginasFood Labelling and Dietary Behaviour Bridging TheSepti Lidya sariAún no hay calificaciones
- 02 01 Methodologies Realizing Potential Hia 2005Documento8 páginas02 01 Methodologies Realizing Potential Hia 2005Lidwina Margaretha LakaAún no hay calificaciones
- From Fringe To Centre Stage: Experiences of Mainstreaming Health Equity in A Health Research CollaborationDocumento14 páginasFrom Fringe To Centre Stage: Experiences of Mainstreaming Health Equity in A Health Research CollaborationAna Porroche-EscuderoAún no hay calificaciones
- Zhang Et Al 2017Documento15 páginasZhang Et Al 2017Mahmoud Abdelfatah MahgoubAún no hay calificaciones
- Innovative Approaches For Improving Maternal and Newborn Health - A Landscape AnalysisDocumento19 páginasInnovative Approaches For Improving Maternal and Newborn Health - A Landscape AnalysisAli Abubakar AuduAún no hay calificaciones
- Nutrition and Physical Activity Programs For Obesity Treatment (PRONAF Study) : Methodological Approach of The ProjectDocumento11 páginasNutrition and Physical Activity Programs For Obesity Treatment (PRONAF Study) : Methodological Approach of The ProjectRodrigo DelgadoAún no hay calificaciones
- ReportDocumento29 páginasReportALNATRON GROUPSAún no hay calificaciones
- Health ProDocumento55 páginasHealth ProMirela ForascuAún no hay calificaciones
- Public Health Dissertation TitlesDocumento7 páginasPublic Health Dissertation TitlesWriteMyPaperPleaseSingapore100% (1)
- Systematic Review Protocol of Interventions To Improve The Psychological Well-Being of General PractitionersDocumento6 páginasSystematic Review Protocol of Interventions To Improve The Psychological Well-Being of General PractitionersKasep PisanAún no hay calificaciones
- Jurnal Cbe 1Documento21 páginasJurnal Cbe 1Dewi SurayaAún no hay calificaciones
- Mobile Paper 1 Mhealth SLR PDFDocumento10 páginasMobile Paper 1 Mhealth SLR PDFJules RosataseAún no hay calificaciones
- Recent Abstracts MPH 65 2020 NUTDocumento3 páginasRecent Abstracts MPH 65 2020 NUTHasriniAún no hay calificaciones
- Final ProposalDocumento20 páginasFinal Proposalapi-293010120Aún no hay calificaciones
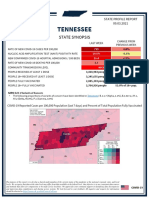
- Tennessee State Profile Report 20210903 PublicDocumento17 páginasTennessee State Profile Report 20210903 PublicAnonymous GF8PPILW5Aún no hay calificaciones
- MSC Project Presentation 29 MarchDocumento36 páginasMSC Project Presentation 29 MarchdreamroseAún no hay calificaciones
- Drug Card MethylcelluloseDocumento2 páginasDrug Card MethylcelluloseAamir AzizAún no hay calificaciones
- Cerebellar StrokeDocumento12 páginasCerebellar StrokewhitecloudsAún no hay calificaciones
- Nurse - Resignation LetterDocumento1 páginaNurse - Resignation LetterphoenixdashAún no hay calificaciones
- Tumors of External EarDocumento10 páginasTumors of External Earsavin1996100% (2)
- 22 Anafilaksise4ed2018Documento52 páginas22 Anafilaksise4ed2018David HartantoAún no hay calificaciones
- asset-v1-UQx BIOIMG101x 1T2016 Type@asset block@BIOIMG101x - SyllabusDocumento8 páginasasset-v1-UQx BIOIMG101x 1T2016 Type@asset block@BIOIMG101x - SyllabusJuhi NeogiAún no hay calificaciones
- First Aid: By: Sem. Winmark S. PerdiganDocumento18 páginasFirst Aid: By: Sem. Winmark S. PerdiganWinsley RazAún no hay calificaciones
- MCH Urology Dissertation TopicsDocumento7 páginasMCH Urology Dissertation TopicsBuyAPaperOnlineBaltimore100% (1)
- Doctor of Veterinary Medicine: 1st Year 1st SemesterDocumento4 páginasDoctor of Veterinary Medicine: 1st Year 1st SemesterDexter LagrimasAún no hay calificaciones
- Celutrat FM EngDocumento2 páginasCelutrat FM EngVíctor Digón TrabadoAún no hay calificaciones
- Management of Perio Prostho Situations in DentistryDocumento18 páginasManagement of Perio Prostho Situations in DentistryHarsha ReddyAún no hay calificaciones
- SOP TEC 15 Calculating Drug Doses v1.1Documento2 páginasSOP TEC 15 Calculating Drug Doses v1.1rajenderizeAún no hay calificaciones
- Pharmacology For Nurses: A Pathophysiologic Approach: Fifth EditionDocumento31 páginasPharmacology For Nurses: A Pathophysiologic Approach: Fifth Editionadni_wgAún no hay calificaciones
- Upper Extremity Reconstruction: Surgical SolutionsDocumento16 páginasUpper Extremity Reconstruction: Surgical Solutionsapi-488115640Aún no hay calificaciones
- Clinical Features of GingivitisDocumento27 páginasClinical Features of Gingivitisfreeda.ampottiAún no hay calificaciones
- Tupoksi & Indikator TO PMDT Prov - Sultra TW3Documento192 páginasTupoksi & Indikator TO PMDT Prov - Sultra TW3AryoWibowoAún no hay calificaciones
- Microbiologist: 3.1.5 Isolation & Gram StainingDocumento5 páginasMicrobiologist: 3.1.5 Isolation & Gram Stainingapi-534896073Aún no hay calificaciones
- Auricular AcupunctureDocumento16 páginasAuricular AcupunctureRamiro GuerreroAún no hay calificaciones
- WHO MHGap Guide English PDFDocumento121 páginasWHO MHGap Guide English PDFYolanda Dwi OktaviyaniAún no hay calificaciones
- Research Paper FinalDocumento7 páginasResearch Paper Finalapi-643588876Aún no hay calificaciones
- IEM MinutesDocumento5 páginasIEM Minutesprasad.dhruv91Aún no hay calificaciones
- Mann Assessment of Swallowing AbilityDocumento9 páginasMann Assessment of Swallowing Abilityluca bastianiAún no hay calificaciones
- Adverse Eventsd DefinitionsDocumento30 páginasAdverse Eventsd Definitionsika sartikaAún no hay calificaciones
- Where There Is No DoctorDocumento503 páginasWhere There Is No DoctorDeborah Mertsch100% (14)
- Practice Nurseled Proactive Care For Chronic Depression in Primary Care A Randomised Controlled TrialDocumento7 páginasPractice Nurseled Proactive Care For Chronic Depression in Primary Care A Randomised Controlled TrialIndah SundariAún no hay calificaciones
- Putney Rehab Centre TimetableDocumento2 páginasPutney Rehab Centre Timetableapi-280584977Aún no hay calificaciones
- AHM Black White Boost FlexiDocumento10 páginasAHM Black White Boost FlexiDani Kirky Ylagan100% (1)
- PPH Simulation PowerpointDocumento1 páginaPPH Simulation Powerpointapi-353926961Aún no hay calificaciones