También podría gustarte
- Primeros Auxilios en Construccion CivilDocumento86 páginasPrimeros Auxilios en Construccion CivilJavier Napoleón Colina Pozo100% (1)
- PRACTICARIO Estructura y Función Humana. 18-1Documento84 páginasPRACTICARIO Estructura y Función Humana. 18-1Ruth Cobo RosalesAún no hay calificaciones
- AIS-APG338 Fractura de La Diafisis Del Cubito y El Radio AdultoDocumento3 páginasAIS-APG338 Fractura de La Diafisis Del Cubito y El Radio Adultoeliana loaizaAún no hay calificaciones
- AIS-APG336 Fractura de EscafoidesDocumento4 páginasAIS-APG336 Fractura de Escafoideseliana loaizaAún no hay calificaciones
- AIS-APG170 Fractura de Tobillo en AdultosDocumento6 páginasAIS-APG170 Fractura de Tobillo en Adultoseliana loaizaAún no hay calificaciones
- AIS-APG169 Fracturas Intertrocantericas de Cadera PDFDocumento3 páginasAIS-APG169 Fracturas Intertrocantericas de Cadera PDFeliana loaizaAún no hay calificaciones
- Lesiones musculo-óseas guíaDocumento24 páginasLesiones musculo-óseas guíaPEDRO LUIS GARCIA ANGARITAAún no hay calificaciones
- Varillas Endomedulares.Documento132 páginasVarillas Endomedulares.Frank ChavezAún no hay calificaciones
- 3 Parcial Traumato CDocumento242 páginas3 Parcial Traumato CAna Gabriela Fernandez Torrez100% (1)
- Avances Tecnológicos en Endodoncia en IrrigaciónDocumento7 páginasAvances Tecnológicos en Endodoncia en IrrigaciónroberthAún no hay calificaciones
- Cirugía Ortopédica en Pequeños AnimalesDocumento35 páginasCirugía Ortopédica en Pequeños AnimalesJuan Sebastian Banoy Forero0% (1)
- FracturaClaviculaTratamientoDocumento71 páginasFracturaClaviculaTratamientoEmmy LiraAún no hay calificaciones
- Ao InfantilDocumento20 páginasAo Infantilfreddydelgado786142Aún no hay calificaciones
- Informe Sobre ReologiaDocumento12 páginasInforme Sobre ReologiaCarlos Andres Peña100% (1)
- Tortura Medicina Forense Jorge OcampoDocumento24 páginasTortura Medicina Forense Jorge OcampoJorge Ocampo100% (1)
- Acumed Surgical Technique ES Clavicle Acu Sinch ESSHD10 02 B PDFDocumento68 páginasAcumed Surgical Technique ES Clavicle Acu Sinch ESSHD10 02 B PDFAngélica VillaAún no hay calificaciones
- Trabajo de Exposicion Primeros AuxiliosDocumento26 páginasTrabajo de Exposicion Primeros AuxiliosMoises GonzalezAún no hay calificaciones
- Lectura 05 Antropología Forense PDFDocumento12 páginasLectura 05 Antropología Forense PDFDebby DiazAún no hay calificaciones
- Traumatismo Naso FacialDocumento2 páginasTraumatismo Naso FacialJOSART ARATH CERNAS ORNELAS100% (1)
- Ortopedia TODODocumento49 páginasOrtopedia TODOMax Guillermo Guzmán MoránAún no hay calificaciones
- Lesiones traumáticas del somaDocumento53 páginasLesiones traumáticas del somaRobert SuizAún no hay calificaciones
- Guia Practica de Fracturas e InmovilizacDocumento18 páginasGuia Practica de Fracturas e Inmovilizacmaria claraAún no hay calificaciones
- Registro de entrega de implementos y charla sobre riesgos laboralesDocumento15 páginasRegistro de entrega de implementos y charla sobre riesgos laboralesFelipe Poblete SaezAún no hay calificaciones
- Medición estrés rocaDocumento14 páginasMedición estrés rocaKatterin CanoAún no hay calificaciones
- Cap OrtopediaDocumento11 páginasCap OrtopediaansatonicoAún no hay calificaciones
- Facitis Plantar - Valoracion y TratamientoDocumento9 páginasFacitis Plantar - Valoracion y TratamientoErnesto Espinosa HookerAún no hay calificaciones
- Guía práctica traumatismos dentales y facialesDocumento46 páginasGuía práctica traumatismos dentales y facialesCecilia de SanctisAún no hay calificaciones
- Clasificaciónes de Fracturas de FemurDocumento2 páginasClasificaciónes de Fracturas de FemurLau Serrano67% (3)
- Desarrollo y CrecimientoDocumento6 páginasDesarrollo y CrecimientoYeroviLisbetteGonzalezGonzalezAún no hay calificaciones
- Fracturas 090719161814 Phpapp01Documento37 páginasFracturas 090719161814 Phpapp01LUZ MONICA VALDIVIESO CLAVIJOAún no hay calificaciones
- Intervencion en Accidente en MontañaDocumento47 páginasIntervencion en Accidente en Montañafervaspaez1Aún no hay calificaciones
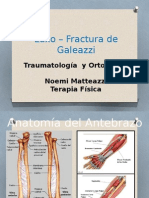
- FX GaleazziDocumento22 páginasFX GaleazziNoemi Matteazzi SpAún no hay calificaciones
- Fracturasdel Tercio Distaldel RadioDocumento47 páginasFracturasdel Tercio Distaldel RadioYasna González MedinaAún no hay calificaciones
- Fracturas expuestas: clasificación y tratamientoDocumento27 páginasFracturas expuestas: clasificación y tratamientojavier patricio cando casanovaAún no hay calificaciones