También podría gustarte
- A Travel Medicine CaseDocumento65 páginasA Travel Medicine CaseDiskta W RonicaAún no hay calificaciones
- Catatonia, Neuroleptic Malignant Syndrome, and Cotard Syndrome in A 22-Year-Old Woman - A Case ReportDocumento3 páginasCatatonia, Neuroleptic Malignant Syndrome, and Cotard Syndrome in A 22-Year-Old Woman - A Case ReportDiskta W RonicaAún no hay calificaciones
- Paediatrica Indonesiana: M. Sholeh Kosim, N.P. Noerpramana, Asril Aminullah, Suharyo HadisaputroDocumento6 páginasPaediatrica Indonesiana: M. Sholeh Kosim, N.P. Noerpramana, Asril Aminullah, Suharyo HadisaputroDiskta W RonicaAún no hay calificaciones
- Diagnosis of Scabies With DermosDocumento2 páginasDiagnosis of Scabies With DermosDiskta W RonicaAún no hay calificaciones
- Diagnosis and Management of Gastroesophageal Reflux Disease (GERD) : An Indian PerspectiveDocumento8 páginasDiagnosis and Management of Gastroesophageal Reflux Disease (GERD) : An Indian PerspectiveDiskta W RonicaAún no hay calificaciones
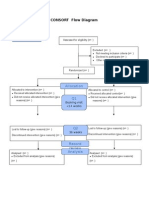
- Additional File 1: CONSORT Flow Diagram: EnrollmentDocumento1 páginaAdditional File 1: CONSORT Flow Diagram: EnrollmentDiskta W RonicaAún no hay calificaciones
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Eapp Las Q3 Week 1Documento8 páginasEapp Las Q3 Week 1Maricel VallejosAún no hay calificaciones
- Q4 SMEA-Sta.-Rosa-IS-HS-S.Y 2021-2022Documento38 páginasQ4 SMEA-Sta.-Rosa-IS-HS-S.Y 2021-2022junapoblacioAún no hay calificaciones
- Construction Skills Learning ExerciseDocumento16 páginasConstruction Skills Learning ExerciseAljaniaAún no hay calificaciones
- ReferencesDocumento12 páginasReferencesBilal RazzaqAún no hay calificaciones
- Social Legislation Cases On Kasambahay LawDocumento12 páginasSocial Legislation Cases On Kasambahay LawLiee Raine100% (1)
- KodalyDocumento11 páginasKodalySally Di Martino100% (3)
- Stock Control Management SyestemDocumento12 páginasStock Control Management SyestemJohn YohansAún no hay calificaciones
- CDP Project InstructionsDocumento6 páginasCDP Project InstructionsNarendra ReddyAún no hay calificaciones
- Forum Discussion #7 UtilitarianismDocumento3 páginasForum Discussion #7 UtilitarianismLisel SalibioAún no hay calificaciones
- Jewellery and ZakatDocumento2 páginasJewellery and ZakatTariq A MalikAún no hay calificaciones
- Revalida ResearchDocumento3 páginasRevalida ResearchJakie UbinaAún no hay calificaciones
- Six Sigma PDFDocumento62 páginasSix Sigma PDFssno1Aún no hay calificaciones
- The 296 Proposed New (Baseline & Monitoring) Methodologies Sent To The Executive BoardDocumento264 páginasThe 296 Proposed New (Baseline & Monitoring) Methodologies Sent To The Executive Boarddjuneja86Aún no hay calificaciones
- (2010) Formulaic Language and Second Language Speech Fluency - Background, Evidence and Classroom Applications-Continuum (2010)Documento249 páginas(2010) Formulaic Language and Second Language Speech Fluency - Background, Evidence and Classroom Applications-Continuum (2010)Như Đặng QuếAún no hay calificaciones
- Banana Oil LabDocumento5 páginasBanana Oil LabjbernayAún no hay calificaciones
- Technical Activities: Ken Goldberg, VP Technical Activities Spring 2007, ICRA, RomeDocumento52 páginasTechnical Activities: Ken Goldberg, VP Technical Activities Spring 2007, ICRA, RomeWasim Ahmad KhanAún no hay calificaciones
- Electrofusion Jointing ProceduresDocumento12 páginasElectrofusion Jointing ProcedureslfpachecoAún no hay calificaciones
- Class 11 Biology Notes Chapter 2 Studyguide360Documento10 páginasClass 11 Biology Notes Chapter 2 Studyguide360AAún no hay calificaciones
- Ethics NotesDocumento99 páginasEthics NotesgowrishhhhAún no hay calificaciones
- Rostam and SohrabDocumento16 páginasRostam and Sohrabronnel100% (1)
- CE GATE'2017 Paper 02 Key Solution PDFDocumento29 páginasCE GATE'2017 Paper 02 Key Solution PDFgolaAún no hay calificaciones
- Lord of The Flies AnalysisDocumento10 páginasLord of The Flies AnalysisMuhammad AsifAún no hay calificaciones
- Budget Anaplan Training DocumentsDocumento30 páginasBudget Anaplan Training DocumentsYudi IfanAún no hay calificaciones
- Rehabilitation Major Repair of Permanent Bridges Bariis Br.Documento2 páginasRehabilitation Major Repair of Permanent Bridges Bariis Br.John Rheynor MayoAún no hay calificaciones
- Lee Meisel 2002 Adsorption and Surface Enhanced Raman of Dyes On Silver and Gold SolsDocumento5 páginasLee Meisel 2002 Adsorption and Surface Enhanced Raman of Dyes On Silver and Gold SolsGabriel FernandesAún no hay calificaciones
- Hard Rock Miner - S Handbook - Jack de La Vergne - Edition 3 - 2003Documento330 páginasHard Rock Miner - S Handbook - Jack de La Vergne - Edition 3 - 2003Adriel senciaAún no hay calificaciones
- Nutrition Science by B Srilakshmi PDFDocumento6 páginasNutrition Science by B Srilakshmi PDFRohan Rewatkar46% (35)
- GOUSGOUNIS Anastenaria & Transgression of The SacredDocumento14 páginasGOUSGOUNIS Anastenaria & Transgression of The Sacredmegasthenis1Aún no hay calificaciones
- Cambridge IGCSE: PHYSICS 0625/63Documento16 páginasCambridge IGCSE: PHYSICS 0625/63...Aún no hay calificaciones
- Human Resource Management in The Hospitality Industry Is FullyDocumento14 páginasHuman Resource Management in The Hospitality Industry Is FullykiahAún no hay calificaciones