También podría gustarte
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Research in Autism Spectrum Disorders: Johnny L. Matson, Jennifer Beighley, Nicole TuryginDocumento6 páginasResearch in Autism Spectrum Disorders: Johnny L. Matson, Jennifer Beighley, Nicole Turyginjhernandez8394Aún no hay calificaciones
- DB MusicDocumento2 páginasDB Musicjhernandez8394Aún no hay calificaciones
- ICD-11 Chapter on Mental DisordersDocumento233 páginasICD-11 Chapter on Mental Disordersedu7683% (6)
- EJ860954Documento7 páginasEJ860954jhernandez8394Aún no hay calificaciones
- Actualizacion Trastornos Del Espectro AutistaDocumento66 páginasActualizacion Trastornos Del Espectro AutistaExodisto PordocimoAún no hay calificaciones
- Señales Tempranas Early IdentificationDocumento33 páginasSeñales Tempranas Early Identificationjhernandez8394Aún no hay calificaciones
- REVIEW 1-S2.0-S0149763413002984-Main PDFDocumento33 páginasREVIEW 1-S2.0-S0149763413002984-Main PDFjhernandez8394Aún no hay calificaciones
- Chown 2016Documento3 páginasChown 2016jhernandez8394Aún no hay calificaciones
- Severe Impairments of Social Interaction PDFDocumento19 páginasSevere Impairments of Social Interaction PDFjhernandez8394100% (1)
- Acidemia Isovalerica y AutismoDocumento5 páginasAcidemia Isovalerica y Autismojhernandez8394Aún no hay calificaciones
- 6th Central Pay Commission Salary CalculatorDocumento15 páginas6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Anna Basso (Auth.), Audrey L. Holland PH.D., Margaret M. Forbes Ph.D. (Eds.) - Aphasia Treatment - World Perspectives-Springer US (1993)Documento384 páginasAnna Basso (Auth.), Audrey L. Holland PH.D., Margaret M. Forbes Ph.D. (Eds.) - Aphasia Treatment - World Perspectives-Springer US (1993)jhernandez8394Aún no hay calificaciones
- Analysis of Gait in Water (Lambeck 2009)Documento56 páginasAnalysis of Gait in Water (Lambeck 2009)jhernandez8394Aún no hay calificaciones
- Cuestionario AsDocumento2 páginasCuestionario Asjhernandez8394Aún no hay calificaciones
- ACIDEMIADocumento5 páginasACIDEMIAjhernandez8394Aún no hay calificaciones
- Bdi 2nu FaqDocumento2 páginasBdi 2nu Faqjhernandez8394Aún no hay calificaciones
- Modelos para El AutismoDocumento22 páginasModelos para El Autismojhernandez8394Aún no hay calificaciones
- Journal of Child Psychology and Psychiatry Volume 39 Issue 1 1998 (Doi 10.1111 - 1469-7610.00301) Susan E. Gathercole - The Development of MemoryDocumento25 páginasJournal of Child Psychology and Psychiatry Volume 39 Issue 1 1998 (Doi 10.1111 - 1469-7610.00301) Susan E. Gathercole - The Development of Memoryjhernandez8394Aún no hay calificaciones
- Behaviors in Students With Autism Four Case StudiesDocumento28 páginasBehaviors in Students With Autism Four Case Studiesjhernandez8394Aún no hay calificaciones
- Journal of Child Psychology and Psychiatry Volume 39 Issue 1 1998 (Doi 10.1111 - 1469-7610.00301) Susan E. Gathercole - The Development of MemoryDocumento25 páginasJournal of Child Psychology and Psychiatry Volume 39 Issue 1 1998 (Doi 10.1111 - 1469-7610.00301) Susan E. Gathercole - The Development of Memoryjhernandez8394Aún no hay calificaciones
- Protocolowisc IV 130103142656 Phpapp02 PDFDocumento16 páginasProtocolowisc IV 130103142656 Phpapp02 PDFelgnavarro344Aún no hay calificaciones
- Applied Cognitive Psychology Volume 13 Issue 1 1999 (Doi 10.1002 - (Sici) 1099-0720 (199902) 13!1!65 - Aid-Acp548 - 3.0.co 2-O) Susan E. Gathercole Elisabet Service Graham J. Hitch Anne-Mar - PhonologDocumento13 páginasApplied Cognitive Psychology Volume 13 Issue 1 1999 (Doi 10.1002 - (Sici) 1099-0720 (199902) 13!1!65 - Aid-Acp548 - 3.0.co 2-O) Susan E. Gathercole Elisabet Service Graham J. Hitch Anne-Mar - Phonologjhernandez8394Aún no hay calificaciones
- Dorothy L. Espelage, Susan M. Swearer Bullying in American Schools A Social-Ecological Perspective On Prevention and Intervention 2003Documento408 páginasDorothy L. Espelage, Susan M. Swearer Bullying in American Schools A Social-Ecological Perspective On Prevention and Intervention 2003jhernandez8394Aún no hay calificaciones
- Increased Brain Activity Dev V SWMDocumento10 páginasIncreased Brain Activity Dev V SWMjhernandez8394Aún no hay calificaciones
- IQ Article Amer Psych March.2012Documento31 páginasIQ Article Amer Psych March.2012jhernandez8394Aún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Skodol Et Al 2011 Part IIDocumento18 páginasSkodol Et Al 2011 Part IIssanagavAún no hay calificaciones
- Neuropsychology in IndiaDocumento16 páginasNeuropsychology in IndiaRahula RakeshAún no hay calificaciones
- Assessment in Counseling: Fourth EditionDocumento16 páginasAssessment in Counseling: Fourth EditionFoxRain08Aún no hay calificaciones
- Diagnosis and Management of Learning Disabilities An Interdisciplinary Lifespan ApproachDocumento244 páginasDiagnosis and Management of Learning Disabilities An Interdisciplinary Lifespan ApproachLilithAún no hay calificaciones
- Psychological AssessmentDocumento5 páginasPsychological AssessmentHeidi BrionesAún no hay calificaciones
- Briere ITCT-A Final PDFDocumento119 páginasBriere ITCT-A Final PDFDave HenehanAún no hay calificaciones
- Whole Person Dementia Assessment (Mast Excerpt)Documento12 páginasWhole Person Dementia Assessment (Mast Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.Aún no hay calificaciones
- Medical Psychology (Tutorial) 2016Documento72 páginasMedical Psychology (Tutorial) 2016Vidhu YadavAún no hay calificaciones
- Reason For Referral: RD THDocumento12 páginasReason For Referral: RD THapi-288903059Aún no hay calificaciones
- VICENTE SOTTO MEDICAL CENTER REPORTSDocumento5 páginasVICENTE SOTTO MEDICAL CENTER REPORTSCarmii HoAún no hay calificaciones
- Review Article 2Documento13 páginasReview Article 2ShreeAún no hay calificaciones
- Iep Writing Guide - 2018 ClcsDocumento29 páginasIep Writing Guide - 2018 Clcsapi-417867603Aún no hay calificaciones
- Gifted Procedures Manual 2018-2019Documento35 páginasGifted Procedures Manual 2018-2019api-483439456Aún no hay calificaciones
- Miller TestDocumento11 páginasMiller Testwillian3219Aún no hay calificaciones
- Drug Education and Vice Control GuideDocumento58 páginasDrug Education and Vice Control GuideRina Cabsaba100% (8)
- Clinical Assessment and Diagnosis: 1) Introduction 2) Basic Elements in Assessment 3) Physical AssessmentDocumento36 páginasClinical Assessment and Diagnosis: 1) Introduction 2) Basic Elements in Assessment 3) Physical AssessmentTrixieCamposano100% (1)
- Sample Chapter 8 Therapeutic ExerciseDocumento29 páginasSample Chapter 8 Therapeutic ExerciseAnsh TanwarAún no hay calificaciones
- MH Disorders: Biological, Emotional, Social AspectsDocumento8 páginasMH Disorders: Biological, Emotional, Social AspectsAndrew BrazzaleAún no hay calificaciones
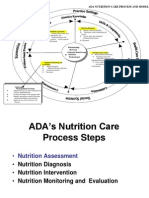
- ADA Nutrition Care Process Model GuideDocumento37 páginasADA Nutrition Care Process Model GuideDadanAún no hay calificaciones
- 6 Fsiqiatria-1524041346Documento48 páginas6 Fsiqiatria-1524041346მირანდა გიორგაშვილიAún no hay calificaciones
- FinalpaperDocumento21 páginasFinalpaperapi-547582127Aún no hay calificaciones
- Nursing Process in Psychiatric NursingDocumento14 páginasNursing Process in Psychiatric NursingJomark Palgan100% (1)
- Job Description Job Details: Psychology Lead Fro Early Intervention, Psychosis Clinical Academic GroupDocumento7 páginasJob Description Job Details: Psychology Lead Fro Early Intervention, Psychosis Clinical Academic GroupRuth Ann HarpurAún no hay calificaciones
- Psychological Assessment GuideDocumento63 páginasPsychological Assessment Guidelailani daya100% (19)
- Individual Differences I: Theories of AbilitiesDocumento29 páginasIndividual Differences I: Theories of AbilitiesHari OmAún no hay calificaciones
- Nursing ProcessDocumento5 páginasNursing ProcessJosal SinonAún no hay calificaciones
- Health Assessment-InterviewDocumento4 páginasHealth Assessment-InterviewMark Elben100% (1)
- The Clinical Interview and AssessmentDocumento6 páginasThe Clinical Interview and AssessmentIoana Antonesi100% (1)
- Psy RatsDocumento11 páginasPsy RatsRavi KumarAún no hay calificaciones
- Who Das 2 Self AdministerednDocumento5 páginasWho Das 2 Self AdministerednJarmy BjAún no hay calificaciones