También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Propofol in NeurotraumaDocumento4 páginasPropofol in NeurotraumaPekerja KesunyianAún no hay calificaciones
- Gcs CommentsDocumento6 páginasGcs CommentsTobyjohn Diapo GemoraAún no hay calificaciones
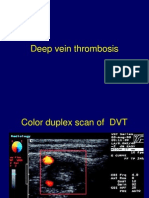
- 2 Deep Vein ThrombosisDocumento10 páginas2 Deep Vein ThrombosisLulu SupergirlAún no hay calificaciones
- Js 09036Documento5 páginasJs 09036Pekerja KesunyianAún no hay calificaciones
- Paul Ridolfi Upper-GIDocumento17 páginasPaul Ridolfi Upper-GIPekerja KesunyianAún no hay calificaciones
- Ccrs 21005Documento12 páginasCcrs 21005Pekerja KesunyianAún no hay calificaciones
- AspergillosisDocumento34 páginasAspergillosisvilla88Aún no hay calificaciones
- A Ann Lumbar SpineDocumento44 páginasA Ann Lumbar SpineAyu SartikaAún no hay calificaciones
- Ccpc13 20 Att2 CRC Slides ProvidersDocumento44 páginasCcpc13 20 Att2 CRC Slides ProvidersPekerja KesunyianAún no hay calificaciones
- 7 - Examination of The AbdomenDocumento48 páginas7 - Examination of The AbdomenPekerja KesunyianAún no hay calificaciones
- Ijav 2012 011-013Documento3 páginasIjav 2012 011-013Pekerja KesunyianAún no hay calificaciones
- Inflammation of the Peritoneal MembraneDocumento16 páginasInflammation of the Peritoneal MembranePekerja KesunyianAún no hay calificaciones
- Ccrs 21031Documento10 páginasCcrs 21031Pekerja KesunyianAún no hay calificaciones
- Ccrs 21023Documento8 páginasCcrs 21023Pekerja KesunyianAún no hay calificaciones
- 105 365 368Documento4 páginas105 365 368Pekerja KesunyianAún no hay calificaciones
- 95 97Documento3 páginas95 97Pekerja KesunyianAún no hay calificaciones
- Ijav 2012 011-013Documento3 páginasIjav 2012 011-013Pekerja KesunyianAún no hay calificaciones
- f167101a-b37b-4feb-b647-3ef5435d02cbDocumento5 páginasf167101a-b37b-4feb-b647-3ef5435d02cbPekerja KesunyianAún no hay calificaciones
- Js 09036Documento5 páginasJs 09036Pekerja KesunyianAún no hay calificaciones
- Daftar PustakaDocumento1 páginaDaftar PustakaPekerja KesunyianAún no hay calificaciones
- 4 - Gangguan - BrainDocumento36 páginas4 - Gangguan - BrainPekerja KesunyianAún no hay calificaciones
- Bone Regenerations - Current Concept and Future DirectionDocumento10 páginasBone Regenerations - Current Concept and Future DirectionPekerja KesunyianAún no hay calificaciones
- Gangguan Pernafasan: Bagian Anestesiologi Dan Reanimasi FK Unsyiah - Rsuza Banda AcehDocumento20 páginasGangguan Pernafasan: Bagian Anestesiologi Dan Reanimasi FK Unsyiah - Rsuza Banda AcehPekerja KesunyianAún no hay calificaciones
- Fracture Healing SsDocumento2 páginasFracture Healing SsIndra SyafaatAún no hay calificaciones
- Gangguan Sirkulasi: Bagian Anestesiologi Dan Reanimasi FK Unsyiah - RSUZA Banda AcehDocumento35 páginasGangguan Sirkulasi: Bagian Anestesiologi Dan Reanimasi FK Unsyiah - RSUZA Banda AcehPekerja KesunyianAún no hay calificaciones
- GmreadmeDocumento1 páginaGmreadmeAccap Aninam DimaraAún no hay calificaciones
- Fracture Healing - The Diamond ConceptDocumento4 páginasFracture Healing - The Diamond ConceptPekerja KesunyianAún no hay calificaciones
- Peritonitis and Intra-Abdominal Abscess Diagnosis TreatmentDocumento16 páginasPeritonitis and Intra-Abdominal Abscess Diagnosis TreatmentPekerja KesunyianAún no hay calificaciones
- 865Documento7 páginas865Pekerja KesunyianAún no hay calificaciones
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- AP PSYCHOLOGY EXAM REVIEW SHEETDocumento6 páginasAP PSYCHOLOGY EXAM REVIEW SHEETNathan HudsonAún no hay calificaciones
- Fruit and Vegetable Diseases PDFDocumento563 páginasFruit and Vegetable Diseases PDFgrigorasalexandru100% (1)
- 10th BIOLOGY PPT CH. NO. 8Documento13 páginas10th BIOLOGY PPT CH. NO. 8Aastha BorhadeAún no hay calificaciones
- Altitude PhysiologyDocumento41 páginasAltitude Physiologyshepherd jeremiahAún no hay calificaciones
- Chapter 4Documento7 páginasChapter 4R LashAún no hay calificaciones
- The Integumentary SystemDocumento11 páginasThe Integumentary SystemHamdy Pagilit DimaporoAún no hay calificaciones
- Blood Buffer SystemDocumento10 páginasBlood Buffer Systemmd hasib munsiAún no hay calificaciones
- Bulacan State University College of Nursing Final Exam ReviewDocumento7 páginasBulacan State University College of Nursing Final Exam ReviewDemiar Madlansacay QuintoAún no hay calificaciones
- NIOSH Investigation - CR 337 Fire LODDDocumento32 páginasNIOSH Investigation - CR 337 Fire LODDRamblingChiefAún no hay calificaciones
- B CellDocumento10 páginasB CellSonia Elizabeth SimonAún no hay calificaciones
- 201305283en Capsurefix 5076Documento2 páginas201305283en Capsurefix 5076Bian PurwaAún no hay calificaciones
- B2 Revision PIXLDocumento26 páginasB2 Revision PIXLtunmishetobilawalAún no hay calificaciones
- Science: Quarter 1 - Module 1Documento10 páginasScience: Quarter 1 - Module 1RUTH PIANGAún no hay calificaciones
- Chapter 6 Cell DivisionDocumento20 páginasChapter 6 Cell DivisionVinash Shka RaoAún no hay calificaciones
- Zoology: Zoology Previous Eamcet QuestionsDocumento8 páginasZoology: Zoology Previous Eamcet QuestionsGaganpreetSingh100% (1)
- UntitledDocumento89 páginasUntitledVladimir VešovićAún no hay calificaciones
- A New Furileusaurian Abelisaurid From La Invernada Upper Cretaceous Santonian Bajo de La Carpa Formation Northern Patagonia ArgentinaDocumento29 páginasA New Furileusaurian Abelisaurid From La Invernada Upper Cretaceous Santonian Bajo de La Carpa Formation Northern Patagonia ArgentinaStuff NewsroomAún no hay calificaciones
- Essential Ayurveda BookDocumento196 páginasEssential Ayurveda BookRoberto89% (9)
- C5 - Metabolism and Enzyme Part 1Documento20 páginasC5 - Metabolism and Enzyme Part 1Daniel LohAún no hay calificaciones
- Phylum Arthropoda - Why such abundance and diversityDocumento4 páginasPhylum Arthropoda - Why such abundance and diversitySHILAún no hay calificaciones
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDocumento14 páginasOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhAún no hay calificaciones
- ICSE Class 10 Biology Previous Year Question Paper 2011 PDFDocumento9 páginasICSE Class 10 Biology Previous Year Question Paper 2011 PDFmohammedAún no hay calificaciones
- The Management of Intra Abdominal Infections From A Global Perspective 2017 WSES Guidelines For Management of Intra Abdominal InfectionsDocumento34 páginasThe Management of Intra Abdominal Infections From A Global Perspective 2017 WSES Guidelines For Management of Intra Abdominal InfectionsJuan CastroAún no hay calificaciones
- Excretory System QuizDocumento17 páginasExcretory System QuizShadab HanafiAún no hay calificaciones
- Auxin Controls Seed Dormacy in Arabidopsis (Liu, Et Al.)Documento6 páginasAuxin Controls Seed Dormacy in Arabidopsis (Liu, Et Al.)Jet Lee OlimberioAún no hay calificaciones
- Wound CareDocumento14 páginasWound CareKirsten Padilla Chua100% (4)
- The Science of Laughing - Worksheet 3Documento3 páginasThe Science of Laughing - Worksheet 3Maria Alexandra PoloAún no hay calificaciones
- He History of ArticulatorsDocumento13 páginasHe History of ArticulatorsrekabiAún no hay calificaciones
- Nicotrol InhalerDocumento19 páginasNicotrol InhalerdebysiskaAún no hay calificaciones
- Circulatory System: Heart, Blood Vessels & Their FunctionsDocumento17 páginasCirculatory System: Heart, Blood Vessels & Their FunctionskangaanushkaAún no hay calificaciones