También podría gustarte
- Orig 1 S 000 Other RDocumento88 páginasOrig 1 S 000 Other Rmayra chipanaAún no hay calificaciones
- Gaviscon Peppermint Liquid Relief - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Documento4 páginasGaviscon Peppermint Liquid Relief - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)edo adimastaAún no hay calificaciones
- Quality Assurance For PharmacyDocumento6 páginasQuality Assurance For PharmacyYetiSamaniegoAún no hay calificaciones
- Mefenamic Acid Public Assessment Report For Pediatric StudiesDocumento17 páginasMefenamic Acid Public Assessment Report For Pediatric StudiesNyoman SuryadinataAún no hay calificaciones
- Neomycin and Prednisolone Acetate Ophthalmic SuspensionDocumento10 páginasNeomycin and Prednisolone Acetate Ophthalmic SuspensionInne Widya UtamiAún no hay calificaciones
- SPC SoludoxDocumento19 páginasSPC SoludoxMihai BirsaAún no hay calificaciones
- ZIOPTAN-taflupros T S Olution/ Drops Akorn, IncDocumento15 páginasZIOPTAN-taflupros T S Olution/ Drops Akorn, IncKamran AlamAún no hay calificaciones
- Miostat InjDocumento4 páginasMiostat InjSri Wahyuni HandayaniAún no hay calificaciones
- Neosporin H Ear DropsDocumento7 páginasNeosporin H Ear DropsRizwan AhmedAún no hay calificaciones
- American Academy of Pediatrics: Abbreviations. Fda, Food and Drug Administration Mdis, Metered-Dose InhalersDocumento13 páginasAmerican Academy of Pediatrics: Abbreviations. Fda, Food and Drug Administration Mdis, Metered-Dose InhalerssylviaAún no hay calificaciones
- Bima To ProstSAKCHBALSKHCVALSHCVDocumento13 páginasBima To ProstSAKCHBALSKHCVALSHCVNonny KhamairaAún no hay calificaciones
- 6 Vol. 1 Issue 3 March 2014 IJP 3244 Paper 6Documento7 páginas6 Vol. 1 Issue 3 March 2014 IJP 3244 Paper 6zalakAún no hay calificaciones
- Drug StudyDocumento14 páginasDrug Studycruz_johnraymond100% (1)
- AlegysalDocumento2 páginasAlegysalhandikaAún no hay calificaciones
- Technological Failures Caused by Cephalexin in Set Type Sheep S Milk YogurtDocumento8 páginasTechnological Failures Caused by Cephalexin in Set Type Sheep S Milk YogurtCarlosAún no hay calificaciones
- OcupolDocumento8 páginasOcupolnada fajriAún no hay calificaciones
- Keto Vs Mikonazol PharmacologyDocumento6 páginasKeto Vs Mikonazol PharmacologyRanda NovalinoAún no hay calificaciones
- Principles of Drug Use During LactationDocumento18 páginasPrinciples of Drug Use During LactationMade SuryaAún no hay calificaciones
- Albumin 20 Per CentDocumento3 páginasAlbumin 20 Per CentidaAún no hay calificaciones
- Monazol, Ovule Spc-EngDocumento6 páginasMonazol, Ovule Spc-EngAhmad Muhammad EmamAún no hay calificaciones
- Albumin (Human) 20%: Presentation ClassificationDocumento3 páginasAlbumin (Human) 20%: Presentation ClassificationZamzam DomaAún no hay calificaciones
- BEPREVE Prescribing InfoDocumento2 páginasBEPREVE Prescribing InfoAnonymous QqyLDoW1Aún no hay calificaciones
- 9% Sodium Chloride Solution MSDSDocumento14 páginas9% Sodium Chloride Solution MSDSbidangAún no hay calificaciones
- Drug Presentation AtropineDocumento6 páginasDrug Presentation AtropineShivam Malik100% (1)
- Drugs and X-Rays For Pregnant and Breastfeeding Women During Dental TreatmentDocumento5 páginasDrugs and X-Rays For Pregnant and Breastfeeding Women During Dental TreatmentArief BudimanAún no hay calificaciones
- 02.ophthalmic Solutions and SuspensionsDocumento7 páginas02.ophthalmic Solutions and SuspensionskhalidAún no hay calificaciones
- Making Medicines That Children Can Take - Nunn - 2003Documento4 páginasMaking Medicines That Children Can Take - Nunn - 2003neutrinomuonAún no hay calificaciones
- Msds Ibuprofen Oral Suspension PDFDocumento7 páginasMsds Ibuprofen Oral Suspension PDFBieGonzAún no hay calificaciones
- The Use of Antifungals: Therapeutics in PracticeDocumento5 páginasThe Use of Antifungals: Therapeutics in PracticeJorge RamirezAún no hay calificaciones
- Buletin Farmasi HRPZDocumento16 páginasBuletin Farmasi HRPZafiq83Aún no hay calificaciones
- CLOBETAZOLDocumento9 páginasCLOBETAZOLJOHA1408Aún no hay calificaciones
- Pharmacy Daily For Fri 04 Jul 2014 - Vaccination Consultation, Fourth Term For Kardachi, MA Warns On Investment, MIMS Updates and Much MoreDocumento3 páginasPharmacy Daily For Fri 04 Jul 2014 - Vaccination Consultation, Fourth Term For Kardachi, MA Warns On Investment, MIMS Updates and Much MorepharmacydailyAún no hay calificaciones
- ProductsafetyassessmentforDexamethasone Sept 2014Documento3 páginasProductsafetyassessmentforDexamethasone Sept 2014azimahakimAún no hay calificaciones
- Thioguanine 20 MG - ML Oral Suspension PDFDocumento4 páginasThioguanine 20 MG - ML Oral Suspension PDFAlexander MeloAún no hay calificaciones
- TbactDocumento7 páginasTbactVinay KumarAún no hay calificaciones
- Drug Use in Pregnancy and Breast FeedingDocumento28 páginasDrug Use in Pregnancy and Breast FeedingStanley Tatenda MukonoAún no hay calificaciones
- Omeprazole 2018: Newborn Use OnlyDocumento5 páginasOmeprazole 2018: Newborn Use OnlyHengky AntonAún no hay calificaciones
- SPC - Vpa22664-150-001Documento5 páginasSPC - Vpa22664-150-001hallaqyara8Aún no hay calificaciones
- Honey and LemonDocumento7 páginasHoney and LemontangxiaomeimayAún no hay calificaciones
- Practical: DR Akshay Dahiwele Assistant Professor JNMC SawangiDocumento54 páginasPractical: DR Akshay Dahiwele Assistant Professor JNMC Sawangiakshay21111985Aún no hay calificaciones
- Brief Summary - Preventing Medication Error in PediatricsDocumento16 páginasBrief Summary - Preventing Medication Error in PediatricsHOD ODAún no hay calificaciones
- MetronidazoleDocumento5 páginasMetronidazoleGwyneth JangadAún no hay calificaciones
- Pregnant or Lactating PatientsDocumento1 páginaPregnant or Lactating PatientsVicentiu PredescuAún no hay calificaciones
- Management of Infection Guidance For Primary Care in IrelandDocumento29 páginasManagement of Infection Guidance For Primary Care in IrelandLouise GleesonAún no hay calificaciones
- Leva FlukeDocumento5 páginasLeva FlukeراجيرحمةربهAún no hay calificaciones
- Pepto - Bismol Rev 2009Documento8 páginasPepto - Bismol Rev 2009martins0105Aún no hay calificaciones
- Parenteral Preparations, Challenges in Formulations Pharmaceutical Outsourcing - The Journal of Pharmaceutical & BiopharmaceutDocumento1 páginaParenteral Preparations, Challenges in Formulations Pharmaceutical Outsourcing - The Journal of Pharmaceutical & BiopharmaceutCRYSTAL A. ARIETAAún no hay calificaciones
- Tamiflu Epar Scientific Discussion enDocumento25 páginasTamiflu Epar Scientific Discussion ensubhasisknkAún no hay calificaciones
- Franco ProfileDocumento46 páginasFranco ProfileSumit SharmaAún no hay calificaciones
- CiprofloxacinDocumento6 páginasCiprofloxacinRasika DaasAún no hay calificaciones
- Drug Study - CefradoxilDocumento13 páginasDrug Study - CefradoxilJohara G'naid0% (1)
- Levocabastine NasalDocumento4 páginasLevocabastine NasalAthiyah IskandarAún no hay calificaciones
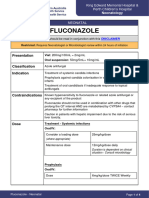
- FluconazoleDocumento4 páginasFluconazoleeucaAún no hay calificaciones
- Heel Descriptive Product Catalogue ENG Oct 2011 8071Documento152 páginasHeel Descriptive Product Catalogue ENG Oct 2011 8071Leandro Daza100% (2)
- MolnupiravirDocumento7 páginasMolnupiravirConcepStore PyAún no hay calificaciones
- Trust FormatDocumento13 páginasTrust FormatMiracle ProsperAún no hay calificaciones
- Beta Karoten: (BAY Ta KARE Oh Teen)Documento9 páginasBeta Karoten: (BAY Ta KARE Oh Teen)Nisa'ul KhoiriyahAún no hay calificaciones
- Ocupol Drops and OintmentDocumento3 páginasOcupol Drops and OintmentAyush KadamAún no hay calificaciones
- Abram Study NotesDocumento6 páginasAbram Study Notesteeman2Aún no hay calificaciones
- Drug Regulatory Affairs: Introduction ToDocumento15 páginasDrug Regulatory Affairs: Introduction ToValentino DhiyuAún no hay calificaciones
- Endemic Rise in Cases of Acute Kidney Injury in Children in Indonesia and Gambia-What Is The Likely Culprit and WhyDocumento4 páginasEndemic Rise in Cases of Acute Kidney Injury in Children in Indonesia and Gambia-What Is The Likely Culprit and WhyValentino DhiyuAún no hay calificaciones
- Pharmaceutical Industry Marketing and InfluenceDocumento84 páginasPharmaceutical Industry Marketing and InfluenceValentino DhiyuAún no hay calificaciones
- Managing Medicine SelectionDocumento16 páginasManaging Medicine SelectionValentino DhiyuAún no hay calificaciones
- Management of Community Pharmacy: Community Pharmacy Is The Place Where Most PharmacistsDocumento32 páginasManagement of Community Pharmacy: Community Pharmacy Is The Place Where Most PharmacistsValentino DhiyuAún no hay calificaciones
- Syllabus of MBA PMDocumento95 páginasSyllabus of MBA PMValentino DhiyuAún no hay calificaciones
- Supply Chain Complexity: A Case Study in The Drive and Control IndustryDocumento186 páginasSupply Chain Complexity: A Case Study in The Drive and Control IndustryValentino DhiyuAún no hay calificaciones
- WHO CHD 98.4dDocumento70 páginasWHO CHD 98.4dValentino DhiyuAún no hay calificaciones
- Crs SCM HealthannexDocumento167 páginasCrs SCM HealthannexValentino DhiyuAún no hay calificaciones
- Development of A Process Analytical TechnologyDocumento8 páginasDevelopment of A Process Analytical TechnologyValentino DhiyuAún no hay calificaciones
- Perfumery Principles Practice-1994Documento348 páginasPerfumery Principles Practice-1994dpaulo7997% (35)
- 31 Days St. Ignatius: Readings To Better Understand St. Ignatius and Ignatian SpiritualityDocumento1 página31 Days St. Ignatius: Readings To Better Understand St. Ignatius and Ignatian SpiritualityValentino DhiyuAún no hay calificaciones
- Binder 2Documento3 páginasBinder 2Valentino DhiyuAún no hay calificaciones
- Total: Quality Management Implementation GuidelinesDocumento83 páginasTotal: Quality Management Implementation GuidelinesValentino DhiyuAún no hay calificaciones
- Stability Assessment of Ketoconazole in Aqueous FormulationsDocumento6 páginasStability Assessment of Ketoconazole in Aqueous FormulationsValentino DhiyuAún no hay calificaciones
- GWI USA Food Trends (1) - 1Documento21 páginasGWI USA Food Trends (1) - 1Valentino DhiyuAún no hay calificaciones
- Fragrance CompositionDocumento5 páginasFragrance CompositionValentino DhiyuAún no hay calificaciones
- Paracetamol Solubility in Pure SolventsDocumento6 páginasParacetamol Solubility in Pure SolventsValentino DhiyuAún no hay calificaciones
- Semisolid FormulationDocumento12 páginasSemisolid FormulationValentino DhiyuAún no hay calificaciones
- Daniel Santiago Rincón PinzónDocumento2 páginasDaniel Santiago Rincón PinzónYANDRA YINNETH RINCON PINZONAún no hay calificaciones
- Hemodynamic Disorders Thromboembolic Disease and ShockDocumento13 páginasHemodynamic Disorders Thromboembolic Disease and ShockAbu HuraraAún no hay calificaciones
- Hepatitis - A - BrochureDocumento2 páginasHepatitis - A - BrochurechategpttrtAún no hay calificaciones
- 11 Anti-Coagulants & FibrinolyticsDocumento52 páginas11 Anti-Coagulants & FibrinolyticsUmmuShefaAún no hay calificaciones
- Small For Gestational AgeDocumento14 páginasSmall For Gestational AgeMaria Delia Salvado100% (2)
- JCC Stemi CompleteDocumento36 páginasJCC Stemi Completeb aAún no hay calificaciones
- b53 Swasa Kosa Mudra 07Documento3 páginasb53 Swasa Kosa Mudra 07shadowfalcon03Aún no hay calificaciones
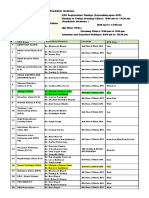
- OPD Schedule DoctorsDocumento3 páginasOPD Schedule DoctorssahilAún no hay calificaciones
- Chapter 3 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Documento25 páginasChapter 3 Hospital Pharmacy Notes Complete Notes by Noteskarts Acc To ER20Shamant TAún no hay calificaciones
- Obstructive Airways Disease: Asthma and COPDDocumento29 páginasObstructive Airways Disease: Asthma and COPDRaxter ErAún no hay calificaciones
- Factitious DisorderDocumento6 páginasFactitious Disorderayu yuliantiAún no hay calificaciones
- 07 Intravenous Immunoglobulin Replacement Therapy in Children With Primary Immunodeficiency Diseases A Nurse S GuideDocumento9 páginas07 Intravenous Immunoglobulin Replacement Therapy in Children With Primary Immunodeficiency Diseases A Nurse S GuidekiminoooAún no hay calificaciones
- AclsDocumento44 páginasAclsArchana GaonkarAún no hay calificaciones
- Nutrition and AIDSDocumento250 páginasNutrition and AIDSLies Pramana SariAún no hay calificaciones
- Score Report - Immunology & Serology at Free Online Quiz SchoolDocumento29 páginasScore Report - Immunology & Serology at Free Online Quiz SchoolThomas GiangAún no hay calificaciones
- Oculofacial ICD-10 Quick Reference As of 100120 FinalDocumento5 páginasOculofacial ICD-10 Quick Reference As of 100120 FinalSelvaganesh KrishnanAún no hay calificaciones
- GERIATRIC HEALTH PresentationDocumento40 páginasGERIATRIC HEALTH Presentationapi-19712253Aún no hay calificaciones
- CDC Interim Reopening GuidanceDocumento62 páginasCDC Interim Reopening GuidanceAlex GeliAún no hay calificaciones
- State of The Art IPDocumento13 páginasState of The Art IPSam SamiAún no hay calificaciones
- Stok 03082022Documento22 páginasStok 03082022Andika SulistiawanAún no hay calificaciones
- Clinical Pharmacy - Introduction - : Prepared By: Dr. C. Suhas ReddyDocumento20 páginasClinical Pharmacy - Introduction - : Prepared By: Dr. C. Suhas Reddysuhas reddyAún no hay calificaciones
- Burns and ScaldsDocumento14 páginasBurns and ScaldsMuhamad IqbalAún no hay calificaciones
- Hyperbaric Oxygen Therapy: ReferenceDocumento5 páginasHyperbaric Oxygen Therapy: ReferenceFariz NurAún no hay calificaciones
- Tutorial 7 Endocrine System II 202001 SDocumento4 páginasTutorial 7 Endocrine System II 202001 SJUN JET LOHAún no hay calificaciones
- Au 31 Mei 2017Documento124 páginasAu 31 Mei 2017Agnes CynthiaAún no hay calificaciones
- Tube FeedingDocumento6 páginasTube FeedingKyla Shain GallegoAún no hay calificaciones
- OB Midwifery Set 1 PDFDocumento9 páginasOB Midwifery Set 1 PDFSquidward Tentacles100% (1)
- Bum Run GradDocumento10 páginasBum Run GradsabyasachiAún no hay calificaciones
- Nursing Diagnosis Handbook by Betty J. Ackley MSN EdS RNDocumento5 páginasNursing Diagnosis Handbook by Betty J. Ackley MSN EdS RNbowagyzeAún no hay calificaciones
- English Drama ScriptDocumento7 páginasEnglish Drama ScriptNadia ASAún no hay calificaciones