También podría gustarte
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Crop RotationsDocumento19 páginasCrop RotationsSarwar M. RasheedAún no hay calificaciones
- Suicide by Cop: Protocol and Training GuideDocumento12 páginasSuicide by Cop: Protocol and Training GuideMichael_Lee_RobertsAún no hay calificaciones
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Survey NotesDocumento166 páginasSurvey Notesglttcgamer100% (1)
- Tanzania Land PolicyDocumento10 páginasTanzania Land PolicyGeorge BulikiAún no hay calificaciones
- Paul Vranas Denver Pit Bull Expert Testimony and Evidence ReviewDocumento4 páginasPaul Vranas Denver Pit Bull Expert Testimony and Evidence ReviewMichael_Lee_Roberts0% (1)
- Re-Engineering Training On Police Use of ForceDocumento84 páginasRe-Engineering Training On Police Use of ForceMichael_Lee_RobertsAún no hay calificaciones
- Topographic Map of ShermanDocumento1 páginaTopographic Map of ShermanHistoricalMaps100% (1)
- Paul Vranas Letter To Denver City Council Re: Pit BullsDocumento1 páginaPaul Vranas Letter To Denver City Council Re: Pit BullsMichael_Lee_RobertsAún no hay calificaciones
- Integrating Communications, Assessment and Tactics (ICAT) Training GuideDocumento72 páginasIntegrating Communications, Assessment and Tactics (ICAT) Training GuideMichael_Lee_Roberts100% (1)
- Question For Grading - 1.9 Questions For Grading - SFSCPX Courseware - EdXDocumento2 páginasQuestion For Grading - 1.9 Questions For Grading - SFSCPX Courseware - EdXwillian01100% (1)
- National Physical Plan PDFDocumento183 páginasNational Physical Plan PDFMeMrAnonymousAún no hay calificaciones
- Colorado Economic and Fiscal Outlook March 2020Documento36 páginasColorado Economic and Fiscal Outlook March 2020Michael_Lee_Roberts100% (1)
- U.S. Supreme Court Petition: Leo Lech, Et Al., v. City of Greenwood Village, Et Al.Documento34 páginasU.S. Supreme Court Petition: Leo Lech, Et Al., v. City of Greenwood Village, Et Al.Michael_Lee_RobertsAún no hay calificaciones
- Lookout Mountain Youth Services Center: Council of Juvenile Correctional Administrators Recommendations With Action StepsDocumento20 páginasLookout Mountain Youth Services Center: Council of Juvenile Correctional Administrators Recommendations With Action StepsMichael_Lee_RobertsAún no hay calificaciones
- Natasha Patnode Settlement AgreementDocumento6 páginasNatasha Patnode Settlement AgreementMichael_Lee_RobertsAún no hay calificaciones
- Officer Susan Mercado: Denver Police Department Order of DisciplineDocumento15 páginasOfficer Susan Mercado: Denver Police Department Order of DisciplineMichael_Lee_RobertsAún no hay calificaciones
- Lookout Mountain Youth Services Center: Council of Juvenile Correctional Administrators ReportDocumento25 páginasLookout Mountain Youth Services Center: Council of Juvenile Correctional Administrators ReportMichael_Lee_RobertsAún no hay calificaciones
- Officer Austin Barela: Denver Police Department Order of DisciplineDocumento15 páginasOfficer Austin Barela: Denver Police Department Order of DisciplineMichael_Lee_RobertsAún no hay calificaciones
- Missing and Murdered Indigenous Women and Girls ReportDocumento28 páginasMissing and Murdered Indigenous Women and Girls ReportMichael_Lee_RobertsAún no hay calificaciones
- Dr. William Moreau Lawsuit Press ReleaseDocumento1 páginaDr. William Moreau Lawsuit Press ReleaseMichael_Lee_RobertsAún no hay calificaciones
- Senate Bill 20-156Documento8 páginasSenate Bill 20-156Michael_Lee_RobertsAún no hay calificaciones
- Mesa County Economic Update, Fourth Quarter 2019Documento13 páginasMesa County Economic Update, Fourth Quarter 2019Michael_Lee_RobertsAún no hay calificaciones
- Estate of Allan George, Et Al., v. City of Rifle, Et Al.Documento20 páginasEstate of Allan George, Et Al., v. City of Rifle, Et Al.Michael_Lee_RobertsAún no hay calificaciones
- Additional Denver Dog Bite Statistics 2019Documento2 páginasAdditional Denver Dog Bite Statistics 2019Michael_Lee_RobertsAún no hay calificaciones
- Brandon Valdez Officer-Involved Shooting Decision LetterDocumento13 páginasBrandon Valdez Officer-Involved Shooting Decision LetterMichael_Lee_RobertsAún no hay calificaciones
- Denver Dog and Cat Bites by Breed 2019Documento2 páginasDenver Dog and Cat Bites by Breed 2019Michael_Lee_RobertsAún no hay calificaciones
- Senate Joint Resolution 20-006Documento7 páginasSenate Joint Resolution 20-006Michael_Lee_RobertsAún no hay calificaciones
- House Bill 20-1014Documento6 páginasHouse Bill 20-1014Michael_Lee_RobertsAún no hay calificaciones
- Denver Public Schools Gender-Neutral Bathrooms ResolutionDocumento3 páginasDenver Public Schools Gender-Neutral Bathrooms ResolutionMichael_Lee_Roberts100% (1)
- Xiaoli Gao and Zhong Wei Zhang IndictmentDocumento12 páginasXiaoli Gao and Zhong Wei Zhang IndictmentMichael_Lee_RobertsAún no hay calificaciones
- Senate Bill 19-091Documento6 páginasSenate Bill 19-091Michael_Lee_RobertsAún no hay calificaciones
- Travis Cook v. City of Arvada, Et Al.Documento19 páginasTravis Cook v. City of Arvada, Et Al.Michael_Lee_RobertsAún no hay calificaciones
- Erik Jensen Sentence Commutation LetterDocumento1 páginaErik Jensen Sentence Commutation LetterMichael_Lee_RobertsAún no hay calificaciones
- House Bill 20-1148Documento3 páginasHouse Bill 20-1148Michael_Lee_RobertsAún no hay calificaciones
- Colorado Senate Bill 20-065Documento7 páginasColorado Senate Bill 20-065Michael_Lee_RobertsAún no hay calificaciones
- Irrigation Scheduling by Book Keeping MethodDocumento13 páginasIrrigation Scheduling by Book Keeping MethodShekh Muhsen Uddin AhmedAún no hay calificaciones
- Farming Life Cycle StepsDocumento6 páginasFarming Life Cycle StepsPurushothaman KAún no hay calificaciones
- RC 001Documento207 páginasRC 001axlmartinoAún no hay calificaciones
- 44746-Thornlands Community Park StagesDocumento1 página44746-Thornlands Community Park StagesCheryl GoodenoughAún no hay calificaciones
- Criteria For Land LevelingDocumento12 páginasCriteria For Land LevelingtizazuAún no hay calificaciones
- Tim Ekberg Co-Ordinator PH 0357273931 Mobile 0427573535: 96 Milawa-Bobinawarrah RD, Milawa, Victoria, 3678Documento5 páginasTim Ekberg Co-Ordinator PH 0357273931 Mobile 0427573535: 96 Milawa-Bobinawarrah RD, Milawa, Victoria, 3678api-25932006Aún no hay calificaciones
- Topographi HQ Topo ReportDocumento8 páginasTopographi HQ Topo ReportslobogeoAún no hay calificaciones
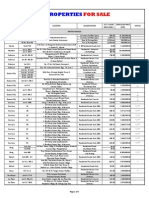
- Ucpb Acquired Assets For Sale - Dec 2013Documento5 páginasUcpb Acquired Assets For Sale - Dec 2013api-239883469Aún no hay calificaciones
- Topographic Map of MaypearlDocumento1 páginaTopographic Map of MaypearlHistoricalMapsAún no hay calificaciones
- Applying New Urbanism Principles to Improve LahoreDocumento3 páginasApplying New Urbanism Principles to Improve LahoreAiman KhurshidAún no hay calificaciones
- Virginia: A Look at AgricultureDocumento1 páginaVirginia: A Look at AgriculturebinkyfishAún no hay calificaciones
- Masbate BL Forms 1st BatchDocumento18 páginasMasbate BL Forms 1st BatchLiezel NibresAún no hay calificaciones
- Residue Management Machinery For CA - Dr. H.S. SidhuDocumento48 páginasResidue Management Machinery For CA - Dr. H.S. SidhuCSISA ProjectAún no hay calificaciones
- Drylands of Balochistan - Kharan DesertDocumento4 páginasDrylands of Balochistan - Kharan DesertGreen Action Sustainable Technology GroupAún no hay calificaciones
- Planting Corn For Grain in TennesseeDocumento3 páginasPlanting Corn For Grain in TennesseeDbaltAún no hay calificaciones
- Site Characterization, Evaluation and Suitability AnalysisDocumento8 páginasSite Characterization, Evaluation and Suitability AnalysisJoni Gabriel CruzataAún no hay calificaciones
- Seminar On Methods of IrrigationDocumento25 páginasSeminar On Methods of IrrigationRavi MalikAún no hay calificaciones
- Boosting Farm Incomes Through Village Cooperative SocietiesDocumento18 páginasBoosting Farm Incomes Through Village Cooperative Societiesprasanthcool100% (2)
- Introduction To AgroforestryDocumento16 páginasIntroduction To AgroforestryBrian JohnsonAún no hay calificaciones
- Strawberry FarmingDocumento1 páginaStrawberry FarmingAJS BATRAAún no hay calificaciones
- (2013) ECLUP Vol.1 Planning Process - HLURBDocumento264 páginas(2013) ECLUP Vol.1 Planning Process - HLURBArnoldAlarcon100% (1)
- Pr.766 400kV QC OHL AP1 - AP28 Tower Schedule (Office (23.04.11)Documento12 páginasPr.766 400kV QC OHL AP1 - AP28 Tower Schedule (Office (23.04.11)Abhinav SinhaAún no hay calificaciones
- Field Trip Report on Forestry and Environmental ScienceDocumento3 páginasField Trip Report on Forestry and Environmental ScienceGourab DaAún no hay calificaciones
- CCFD 2012 Delinquent Residential Taxes PDFDocumento15 páginasCCFD 2012 Delinquent Residential Taxes PDFCovGansettSKPatch0% (1)