También podría gustarte
- Basic Ethical Principles in HealthcareDocumento6 páginasBasic Ethical Principles in HealthcareRegine Lorenzana Mey-Ang100% (1)
- Atlas of Critical Care EchocardiographyDocumento189 páginasAtlas of Critical Care EchocardiographyAnna Anna100% (1)
- Antiviral Drugs Classification and MechanismsDocumento56 páginasAntiviral Drugs Classification and MechanismsciccianoAún no hay calificaciones
- FNCP Form Health Deficit AsthmaDocumento3 páginasFNCP Form Health Deficit Asthmakappa100% (1)
- Coronary Artery Disease PathophysiologyDocumento3 páginasCoronary Artery Disease Pathophysiologynursing concept maps67% (3)
- Fecalysis: Tests on Stool Samples to Diagnose Digestive ConditionsDocumento2 páginasFecalysis: Tests on Stool Samples to Diagnose Digestive ConditionsHan SoloAún no hay calificaciones
- The Immune SystemDocumento17 páginasThe Immune SystemMostafa Galal El Din100% (1)
- Bio 2 Quiz ReviewerDocumento2 páginasBio 2 Quiz ReviewerAlexandra RoderoAún no hay calificaciones
- Cardiac RehabilitationDocumento5 páginasCardiac RehabilitationGian Carlo Poggi EscobarAún no hay calificaciones
- Multiple Sclerosis Concept MapDocumento1 páginaMultiple Sclerosis Concept MapKyle Santos50% (2)
- COURSE UNIT - CU5 Nurses Role in Disaster Part 2 - Copy-2Documento4 páginasCOURSE UNIT - CU5 Nurses Role in Disaster Part 2 - Copy-2Danica FrancoAún no hay calificaciones
- Prelim Funda Lec Transes CompleteDocumento42 páginasPrelim Funda Lec Transes CompleteLoLiAún no hay calificaciones
- Haloperidol Drug StudyDocumento2 páginasHaloperidol Drug StudyNajmah Saaban100% (5)
- Nursing Care for Patients with Immune DisordersDocumento7 páginasNursing Care for Patients with Immune DisordersIrish Eunice FelixAún no hay calificaciones
- Organization of Immune SystemDocumento44 páginasOrganization of Immune SystemSaubie AslamiahAún no hay calificaciones
- Answers To The Cambridge Checkpoint Science 2Documento28 páginasAnswers To The Cambridge Checkpoint Science 2Nur Dina ZaulkifleeAún no hay calificaciones
- Immune FunctionDocumento27 páginasImmune Functionhalloween candyAún no hay calificaciones
- CestodesDocumento83 páginasCestodesveralynn2011Aún no hay calificaciones
- Overview of Immune ResponsesDocumento30 páginasOverview of Immune ResponsesVivien KasimAún no hay calificaciones
- Test Bank For Little and Falaces Dental Management of The Medically Compromised Patient 9th EditionDocumento3 páginasTest Bank For Little and Falaces Dental Management of The Medically Compromised Patient 9th EditionAddison Rogers100% (35)
- Acute InflammationDocumento55 páginasAcute InflammationMohammad_Islam8790% (10)
- Drug StudyDocumento6 páginasDrug StudyNajmah Saaban100% (1)
- Rheumatic FeverDocumento56 páginasRheumatic Feveralmawang100% (1)
- Pass PACES in Single AttemptDocumento101 páginasPass PACES in Single AttemptSOMNATHAún no hay calificaciones
- Delayed Hypersensitivity and Type IV ReactionsDocumento12 páginasDelayed Hypersensitivity and Type IV Reactionsella Sy100% (1)
- Immune Responses: Introduction to Innate and Adaptive ImmunityDocumento10 páginasImmune Responses: Introduction to Innate and Adaptive ImmunityArvi MandaweAún no hay calificaciones
- Pathophy of Appendicitis (Or) by Mizzy BaylonDocumento2 páginasPathophy of Appendicitis (Or) by Mizzy BaylonmizzybaylonAún no hay calificaciones
- Immunologic Disorders ExplainedDocumento73 páginasImmunologic Disorders ExplainedDjayAún no hay calificaciones
- Bisacodyl (Dolculax-Biscolax) Drug StudyDocumento1 páginaBisacodyl (Dolculax-Biscolax) Drug StudyNajmah Saaban0% (1)
- Risperidone Drug StudyDocumento2 páginasRisperidone Drug StudyNajmah Saaban77% (13)
- Week 2-3 Part 1Documento26 páginasWeek 2-3 Part 1EmpieAún no hay calificaciones
- Understanding the Immune System and Its FunctionsDocumento51 páginasUnderstanding the Immune System and Its FunctionsZin LimAún no hay calificaciones
- B. Pathophysiology: Clinical Aspects of Cancer DiagnosisDocumento10 páginasB. Pathophysiology: Clinical Aspects of Cancer DiagnosisAbigael Patricia GutierrezAún no hay calificaciones
- Immunology - Nursing HandoutsDocumento22 páginasImmunology - Nursing HandoutsRayePrudente100% (1)
- Pneumonia and TuberculosisDocumento18 páginasPneumonia and TuberculosisVincent QuitorianoAún no hay calificaciones
- Hemophilia Nursing CareDocumento10 páginasHemophilia Nursing CareEla 15Aún no hay calificaciones
- NCM 112: Care of Client With Inflammatory and Immunologic ResponseDocumento10 páginasNCM 112: Care of Client With Inflammatory and Immunologic ResponseNikitaCaitlynLeyaleyAún no hay calificaciones
- Innate and Adaptive Immunity: Cells, Organs and FunctionsDocumento17 páginasInnate and Adaptive Immunity: Cells, Organs and FunctionsBasma RagabAún no hay calificaciones
- NCM 112 Lecture NotesDocumento5 páginasNCM 112 Lecture NotesSureen RegularAún no hay calificaciones
- Sci9 Q1 Mod2 Effects of Lifestyle On The Respiratory and Circulatory Systems Version3 Edited3Documento23 páginasSci9 Q1 Mod2 Effects of Lifestyle On The Respiratory and Circulatory Systems Version3 Edited3NOVA LESLIE AGAPAYAún no hay calificaciones
- Rabies Virus, Disease, and PreventionDocumento25 páginasRabies Virus, Disease, and PreventionAdindapauliaAún no hay calificaciones
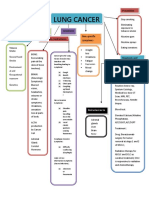
- Concept Map LungDocumento1 páginaConcept Map LungThea Eya FayeAún no hay calificaciones
- Prelims - GMJ Lecture - Module 2 III DisorderDocumento5 páginasPrelims - GMJ Lecture - Module 2 III DisorderjuiceAún no hay calificaciones
- Assessment of Immune FunctionDocumento3 páginasAssessment of Immune Functionhalloween candyAún no hay calificaciones
- Topic 3 NCM 112Documento4 páginasTopic 3 NCM 112Marielle ChuaAún no hay calificaciones
- September 13 - NCM 112 (Mam G)Documento2 páginasSeptember 13 - NCM 112 (Mam G)Aaron DayloAún no hay calificaciones
- Anatomy Ch. 9 The Senses NotesDocumento7 páginasAnatomy Ch. 9 The Senses Notesprincepalestine100% (1)
- NCP 2 Impaired Skin Integrity EDITEDDocumento2 páginasNCP 2 Impaired Skin Integrity EDITEDVincent HermanoAún no hay calificaciones
- NCM 104 - RleDocumento25 páginasNCM 104 - RleAbigael Patricia GutierrezAún no hay calificaciones
- Different Types of VaccinesDocumento4 páginasDifferent Types of VaccinesTenisha KnowlesAún no hay calificaciones
- Complement SystemDocumento6 páginasComplement SystemJimit GandhiAún no hay calificaciones
- Hematology: - The Science Dealing With The FormationDocumento104 páginasHematology: - The Science Dealing With The FormationYamSomandarAún no hay calificaciones
- Pharma Trans Le1Documento60 páginasPharma Trans Le1Kunal TribhuvanAún no hay calificaciones
- Concepts in Immunologic Function: Chapter 35: Assessment of Immune FunctionDocumento9 páginasConcepts in Immunologic Function: Chapter 35: Assessment of Immune FunctionKristine KimAún no hay calificaciones
- Iv. Review of Anatomy and Physiology Figure 1. The Immune SystemDocumento7 páginasIv. Review of Anatomy and Physiology Figure 1. The Immune SystemNejie Zarrah Diaz100% (1)
- NematodaDocumento96 páginasNematodaPurplesmilezAún no hay calificaciones
- Immune SystemDocumento10 páginasImmune Systemailyn regaladoAún no hay calificaciones
- Anatomy and Physiology SLEDocumento27 páginasAnatomy and Physiology SLEMoti Pagador100% (4)
- Hematologic ProblemsDocumento26 páginasHematologic Problemsapi-3735995100% (2)
- Pa Tho Physiology Part 1Documento1 páginaPa Tho Physiology Part 1anonymous89ify100% (2)
- Blood and Tissue FlagellatesDocumento5 páginasBlood and Tissue FlagellatesChristine BuenAún no hay calificaciones
- General Pathology For Medical StudentsDocumento225 páginasGeneral Pathology For Medical Studentsscousevet100% (1)
- Chapter 13 Diagnosing Infectious DiseasesDocumento47 páginasChapter 13 Diagnosing Infectious DiseasesSherinne Jane CariazoAún no hay calificaciones
- Entamoeba ColiDocumento14 páginasEntamoeba ColiHanisha Erica100% (1)
- Infectios DiseasesDocumento183 páginasInfectios DiseasesAnonymous eson90Aún no hay calificaciones
- Proper Excreta Disposal, Food Safety and Environmental HealthDocumento15 páginasProper Excreta Disposal, Food Safety and Environmental HealthEden LacsonAún no hay calificaciones
- Amoebiasis Symptoms, Causes, Treatment and PreventionDocumento8 páginasAmoebiasis Symptoms, Causes, Treatment and PreventionJamie JunioAún no hay calificaciones
- Chapter 5: Normal Flora of The Human BodyDocumento3 páginasChapter 5: Normal Flora of The Human BodyNicole NipasAún no hay calificaciones
- Anatomy and physiology of bloodDocumento4 páginasAnatomy and physiology of bloodDylle Lorenzo ClaudioAún no hay calificaciones
- 10 - Defenses Against Disease - Week8 - DrNyembe - 2022Documento26 páginas10 - Defenses Against Disease - Week8 - DrNyembe - 2022Muke MpilwenhleAún no hay calificaciones
- IMMUNITYDocumento23 páginasIMMUNITYFlorence Lynn BaisacAún no hay calificaciones
- Immunology ImmunologyDocumento136 páginasImmunology ImmunologyZeen_Zeen_Fern_3128Aún no hay calificaciones
- Aminoleban Drug StudyDocumento1 páginaAminoleban Drug StudyNajmah Saaban100% (1)
- Gouty Arthritis Diagnostic TestsDocumento7 páginasGouty Arthritis Diagnostic TestsNajmah SaabanAún no hay calificaciones
- Juvenile Arthritis Diagnostic TestsDocumento5 páginasJuvenile Arthritis Diagnostic TestsNajmah SaabanAún no hay calificaciones
- Ross' Ethical Theory (Assignment)Documento3 páginasRoss' Ethical Theory (Assignment)Najmah SaabanAún no hay calificaciones
- Myocardial InfarctionDocumento34 páginasMyocardial InfarctionMeera ANN AJIAún no hay calificaciones
- MPAS540 2019 PA Medicine I SyllabusDocumento6 páginasMPAS540 2019 PA Medicine I SyllabusSteven CongressAún no hay calificaciones
- BRS Anatomy - Thorax Flashcards by Grace Caldwell - BrainscapeDocumento45 páginasBRS Anatomy - Thorax Flashcards by Grace Caldwell - BrainscapeCarmela MarianoAún no hay calificaciones
- Poisoning - Environmental Exposure (Medicalstudyzone - Com)Documento95 páginasPoisoning - Environmental Exposure (Medicalstudyzone - Com)Roshan MevadaAún no hay calificaciones
- MCQ PaperDocumento23 páginasMCQ PaperJapleen SinghAún no hay calificaciones
- RPT Science Form 3 2020 NEW NORM PDFDocumento66 páginasRPT Science Form 3 2020 NEW NORM PDFIbtisyam Ab RahimAún no hay calificaciones
- Polytrauma EARLY MX 2009Documento87 páginasPolytrauma EARLY MX 2009Fina Syafinaz SuhaimiAún no hay calificaciones
- MCQ PretestDocumento3 páginasMCQ PretestKia AgusputraAún no hay calificaciones
- Full Download Test Bank For Ecg Essentials of Electrocardiography 1st Edition by Soto PDF Full ChapterDocumento21 páginasFull Download Test Bank For Ecg Essentials of Electrocardiography 1st Edition by Soto PDF Full Chapteradrianblackiadxetkrqm100% (12)
- Human Cardiovascular System: Introduction ToDocumento76 páginasHuman Cardiovascular System: Introduction ToJunje SemeonAún no hay calificaciones
- Annicchiaricopetruzzelli Thesis 2017Documento90 páginasAnnicchiaricopetruzzelli Thesis 2017Lia SantillanAún no hay calificaciones
- Gr. 9 Science LM (AG)Documento33 páginasGr. 9 Science LM (AG)Aizalonica GalangAún no hay calificaciones
- Cardiovascular System: PBL Batch 2020Documento484 páginasCardiovascular System: PBL Batch 2020Caroline AgathaAún no hay calificaciones
- Coronary Artery Disease Diagnosis and TreatmentDocumento56 páginasCoronary Artery Disease Diagnosis and TreatmentwiwiAún no hay calificaciones
- Flash CardsDocumento35 páginasFlash CardsMihaela AlexandraAún no hay calificaciones
- Mitral Annular Disjunction: A Systematic Review of The LiteratureDocumento10 páginasMitral Annular Disjunction: A Systematic Review of The LiteratureAlznoskillAún no hay calificaciones
- MegaCode and Team Management ACLS AHADocumento7 páginasMegaCode and Team Management ACLS AHAEunice PalloganAún no hay calificaciones
- Pru TermDocumento6 páginasPru TermJaboh LabohAún no hay calificaciones
- Circulatory SystemDocumento6 páginasCirculatory SystemMN NgọcAún no hay calificaciones
- Overview CurriculumDocumento23 páginasOverview CurriculumMaria EdelAún no hay calificaciones
- Regulation of Cardiac Output and Venous Return by Dr. RoomiDocumento44 páginasRegulation of Cardiac Output and Venous Return by Dr. RoomiMudassar RoomiAún no hay calificaciones
- Evolving Indications For Permanent PacemakersDocumento12 páginasEvolving Indications For Permanent PacemakersJazmín Alejandra AGAún no hay calificaciones