También podría gustarte
- Newman's Billing and Coding Technicians Study GuideDe EverandNewman's Billing and Coding Technicians Study GuideCalificación: 4.5 de 5 estrellas4.5/5 (2)
- Newman's Medical Billing and Coding Technicians Study GuideDe EverandNewman's Medical Billing and Coding Technicians Study GuideAún no hay calificaciones
- Billing Definations 7Documento15 páginasBilling Definations 7Saeed ahmed100% (1)
- Healthcare GlossaryDocumento18 páginasHealthcare GlossaryKalagara Mohan KrishnaAún no hay calificaciones
- IV Study Guide 2013Documento78 páginasIV Study Guide 2013Kaloy KamaoAún no hay calificaciones
- Outpatient Care Facilities Regulation - DubaiDocumento68 páginasOutpatient Care Facilities Regulation - DubaiMustaphaAún no hay calificaciones
- Jci Ambulatory Care 3e Standards OnlyDocumento41 páginasJci Ambulatory Care 3e Standards OnlyAhmed100% (1)
- Textbook of Urgent Care Management: Chapter 40, Implementing Occupational MedicineDe EverandTextbook of Urgent Care Management: Chapter 40, Implementing Occupational MedicineAún no hay calificaciones
- Referral PolicyDocumento5 páginasReferral PolicyJan Oneille Y. Valles100% (1)
- U.S. Tax Court Findings of Fraud On Tax Returns by Curt AnkerbergDocumento8 páginasU.S. Tax Court Findings of Fraud On Tax Returns by Curt AnkerbergMail TribuneAún no hay calificaciones
- Documentation of Medical Evidence For Disability Evaluation PurposesDocumento5 páginasDocumentation of Medical Evidence For Disability Evaluation PurposesJim100% (2)
- Att Usa PDFDocumento3 páginasAtt Usa PDFČårl-Ünløćkēr EdouardAún no hay calificaciones
- Memorandum of AgreementDocumento3 páginasMemorandum of AgreementjenelleAún no hay calificaciones
- BANK CONFIRMATION AUDITDocumento7 páginasBANK CONFIRMATION AUDITZulu198005Aún no hay calificaciones
- Guidelines For ICU Admission, Discharge, and Triage (Crit Care Med 1999)Documento11 páginasGuidelines For ICU Admission, Discharge, and Triage (Crit Care Med 1999)Kary VelazquezAún no hay calificaciones
- White Paper TelemedicineDocumento8 páginasWhite Paper TelemedicineKamau GabrielAún no hay calificaciones
- Ambulatory Service Center Pro FormaDocumento20 páginasAmbulatory Service Center Pro FormajorhnAún no hay calificaciones
- Guide To Infection Prevention in Outpatient Settings: Minimum Expectations For Safe CareDocumento16 páginasGuide To Infection Prevention in Outpatient Settings: Minimum Expectations For Safe CareJun AnteolaAún no hay calificaciones
- Hospital RegulationDocumento97 páginasHospital RegulationKarthikeyan JothiramalingamAún no hay calificaciones
- Surgical Self-Assessment ChecklistDocumento8 páginasSurgical Self-Assessment ChecklistJyoti KumarAún no hay calificaciones
- Jciamb4th Standards OnlyDocumento25 páginasJciamb4th Standards OnlyZeeshan AliAún no hay calificaciones
- John Bala MapsDocumento3 páginasJohn Bala MapsJayson80% (10)
- Guidebook For Hospitals - 4th EditionDocumento239 páginasGuidebook For Hospitals - 4th EditionJobin JamesAún no hay calificaciones
- Activos FijosDocumento28 páginasActivos FijosArelyAún no hay calificaciones
- VHA Directive Requires Notification of Medical Staff Involved in Malpractice ClaimsDocumento13 páginasVHA Directive Requires Notification of Medical Staff Involved in Malpractice ClaimsArvin TerrellAún no hay calificaciones
- Medicare Claims Processing Manual: Chapter 35 - Independent Diagnostic Testing Facility (IDTF)Documento7 páginasMedicare Claims Processing Manual: Chapter 35 - Independent Diagnostic Testing Facility (IDTF)sekhar babuAún no hay calificaciones
- Overview of Hospital Utilization Review Legal AuthorityDocumento5 páginasOverview of Hospital Utilization Review Legal AuthoritybambangAún no hay calificaciones
- AAPM R Comments On Proposed Review Choice Demonstration For Inpatient Rehabilitation Facility ServicesDocumento15 páginasAAPM R Comments On Proposed Review Choice Demonstration For Inpatient Rehabilitation Facility ServicesKhalil KhusairiAún no hay calificaciones
- HealthcareDocumento14 páginasHealthcareAntony AjowiAún no hay calificaciones
- Credentialing - WikipediaDocumento5 páginasCredentialing - WikipediaYetti DarmiAún no hay calificaciones
- DOH Standard for Emergency CareDocumento21 páginasDOH Standard for Emergency CareMendero Medical CenterAún no hay calificaciones
- Che 262 Referral System and Outreach ServicesDocumento12 páginasChe 262 Referral System and Outreach ServicesArum ComradeAún no hay calificaciones
- Critical Deficiencies at The Washington DC VA Medical CenterDocumento158 páginasCritical Deficiencies at The Washington DC VA Medical CenterAllison MaassAún no hay calificaciones
- JB Pritzker, Governor Ngozi O. Ezike, MD, DirectorDocumento20 páginasJB Pritzker, Governor Ngozi O. Ezike, MD, DirectorNewsTeam20Aún no hay calificaciones
- Medicare Reimbursement For Nurse Practitioners in Long-Term CareDocumento23 páginasMedicare Reimbursement For Nurse Practitioners in Long-Term CareOMGStudy0% (1)
- Elective Surgery Policy v3.0Documento3 páginasElective Surgery Policy v3.0halosunyrtimr6Aún no hay calificaciones
- Health Information Exchange 101:: Important Terms and DefinitionsDocumento71 páginasHealth Information Exchange 101:: Important Terms and DefinitionsSuccessEHSAún no hay calificaciones
- Cigna'S Preventive Health Coverage: A Guide ToDocumento12 páginasCigna'S Preventive Health Coverage: A Guide TomcrphAún no hay calificaciones
- DHA Health Facility Guidelines 2019: Part B - Health Facility Briefing & Design 20 - Admissions Unit & DischargeDocumento30 páginasDHA Health Facility Guidelines 2019: Part B - Health Facility Briefing & Design 20 - Admissions Unit & Dischargechandan guptaAún no hay calificaciones
- Managed CareDocumento5 páginasManaged CareMutia Poetry MandelaAún no hay calificaciones
- Clinical Activity History ReportDocumento2 páginasClinical Activity History ReportshahidAún no hay calificaciones
- 2007 National Patient Safety Goals: For Those Programs Required To Complete A PPRDocumento11 páginas2007 National Patient Safety Goals: For Those Programs Required To Complete A PPRKenny JosefAún no hay calificaciones
- Outpatient Services Implementation Standard: 1. PurposeDocumento20 páginasOutpatient Services Implementation Standard: 1. PurposeReginaAstariTjoegitoAún no hay calificaciones
- LTC-Hospital Collaboration to Prevent HAC ConditionsDocumento2 páginasLTC-Hospital Collaboration to Prevent HAC Conditionskudo01Aún no hay calificaciones
- Parivar Mediclaim Policy 17 B (I)Documento11 páginasParivar Mediclaim Policy 17 B (I)RKAún no hay calificaciones
- Solution Manual For Comparative Health Information Management 4th Edition by Peden ISBN 1285871715 9781285871714Documento9 páginasSolution Manual For Comparative Health Information Management 4th Edition by Peden ISBN 1285871715 9781285871714jaredhernandezbazicwejqt100% (28)
- Peace Corps Certified Nurses Practioner Physician AssistantDocumento15 páginasPeace Corps Certified Nurses Practioner Physician AssistantAccessible Journal Media: Peace Corps DocumentsAún no hay calificaciones
- Revisions To Interpretive Guidelines For Centers For Medicare & Medicaid Services Hospital Conditions of Participation 42 CFR 482.12, 482.13, 482.27 and 482.28Documento12 páginasRevisions To Interpretive Guidelines For Centers For Medicare & Medicaid Services Hospital Conditions of Participation 42 CFR 482.12, 482.13, 482.27 and 482.28Beverly TranAún no hay calificaciones
- Guide To Infection Prevention For Outpatient Settings:: Minimum Expectations For Safe CareDocumento42 páginasGuide To Infection Prevention For Outpatient Settings:: Minimum Expectations For Safe Caresalcais9042Aún no hay calificaciones
- Guide infection prevention outpatient careDocumento42 páginasGuide infection prevention outpatient careAli GhanemAún no hay calificaciones
- Fact Sheet: Medicare Federally Qualified Health Center Advanced Primary Care Practice DemonstrationDocumento6 páginasFact Sheet: Medicare Federally Qualified Health Center Advanced Primary Care Practice Demonstrationapi-94302037Aún no hay calificaciones
- HIM 200 Final Project6Documento10 páginasHIM 200 Final Project6Robin McFaddenAún no hay calificaciones
- Ahmed Linkage PresentationDocumento15 páginasAhmed Linkage PresentationKRUSU ISAACAún no hay calificaciones
- Peace Corps PCMC SOW REGISTERED NURSEDocumento9 páginasPeace Corps PCMC SOW REGISTERED NURSEAccessible Journal Media: Peace Corps DocumentsAún no hay calificaciones
- CHHS Clinical Handover ProcedureDocumento16 páginasCHHS Clinical Handover ProcedureSiu Andrea100% (1)
- Videoconferenced Telebehavioral Health Referral Process AdherenceDocumento7 páginasVideoconferenced Telebehavioral Health Referral Process AdherenceCarolina UrrutiaAún no hay calificaciones
- NABH 3rd EditionDocumento259 páginasNABH 3rd Edition19112281s3785Aún no hay calificaciones
- Online Healthcare System for Outpatient RecordsDocumento42 páginasOnline Healthcare System for Outpatient RecordsFMTech ConsultsAún no hay calificaciones
- Minnesota Guidelines For Resuming Time Sensitive Surgery and Procedures: COVID-19 BackgroundDocumento5 páginasMinnesota Guidelines For Resuming Time Sensitive Surgery and Procedures: COVID-19 BackgroundJill BurcumAún no hay calificaciones
- Vhaoemseniorstaff@Va GovDocumento17 páginasVhaoemseniorstaff@Va Govchris.lucasAún no hay calificaciones
- Application Quick Guide: ET3 Model Medical Triage Line Notice of Funding Opportunity (NOFO)Documento3 páginasApplication Quick Guide: ET3 Model Medical Triage Line Notice of Funding Opportunity (NOFO)epraetorianAún no hay calificaciones
- Medical Billing QuestionnDocumento10 páginasMedical Billing QuestionnZulqarnain HaiderAún no hay calificaciones
- Chapter 02Documento44 páginasChapter 02Carlos ChuAún no hay calificaciones
- Standards For Outpatient Clinical ServicesDocumento10 páginasStandards For Outpatient Clinical Servicessaintiyke58Aún no hay calificaciones
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipDe EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipAún no hay calificaciones
- B: COVID-19 O: Rief Report Epidemic Trends and Projections in RegonDocumento18 páginasB: COVID-19 O: Rief Report Epidemic Trends and Projections in RegonMail TribuneAún no hay calificaciones
- Gov. Kate Brown's Letter - Jackson County Reopening, Phase 1Documento1 páginaGov. Kate Brown's Letter - Jackson County Reopening, Phase 1Mail TribuneAún no hay calificaciones
- Jackson County Phase 2 Letter of ApprovalDocumento1 páginaJackson County Phase 2 Letter of ApprovalMail TribuneAún no hay calificaciones
- RCC's Design 4 Change MagazineDocumento24 páginasRCC's Design 4 Change MagazineMail Tribune100% (1)
- COVID-19 Intervention Effectiveness and Epidemic Trends For Oregon: A Model-Based AnalysisDocumento10 páginasCOVID-19 Intervention Effectiveness and Epidemic Trends For Oregon: A Model-Based AnalysisMail TribuneAún no hay calificaciones
- 2020 06 01 PhaseII Plan Letter FINALDocumento12 páginas2020 06 01 PhaseII Plan Letter FINALMail TribuneAún no hay calificaciones
- Roger Stone EndorsementDocumento1 páginaRoger Stone EndorsementMail TribuneAún no hay calificaciones
- Medford Community OutreachDocumento30 páginasMedford Community OutreachMail TribuneAún no hay calificaciones
- DEQ Jordan Cove Evaluation ReportDocumento209 páginasDEQ Jordan Cove Evaluation ReportMail TribuneAún no hay calificaciones
- 2018-19 Oregon School Boards Association Salary Survey BookDocumento137 páginas2018-19 Oregon School Boards Association Salary Survey BookMail TribuneAún no hay calificaciones
- Jackson County ProclamationDocumento2 páginasJackson County ProclamationMail TribuneAún no hay calificaciones
- DEQ Jordan Cove Evaluation ReportDocumento209 páginasDEQ Jordan Cove Evaluation ReportMail TribuneAún no hay calificaciones
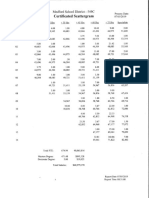
- Medford Teacher Salary ScattergramDocumento1 páginaMedford Teacher Salary ScattergramMail TribuneAún no hay calificaciones
- Phoenix-Talent School Board Student Investment Account PresentationDocumento14 páginasPhoenix-Talent School Board Student Investment Account PresentationMail TribuneAún no hay calificaciones
- Medford School District Capital Project & Communication AnalysisDocumento81 páginasMedford School District Capital Project & Communication AnalysisMail TribuneAún no hay calificaciones
- Letter To PEA PresidentDocumento1 páginaLetter To PEA PresidentMail TribuneAún no hay calificaciones
- Bankruptcy Complaint Prior To Plane CrashDocumento8 páginasBankruptcy Complaint Prior To Plane CrashMail TribuneAún no hay calificaciones
- 2019-20 Proposed Budget Presentation 042919Documento48 páginas2019-20 Proposed Budget Presentation 042919Mail TribuneAún no hay calificaciones
- District Attorney's Report On Police Shooting in Eagle PointDocumento3 páginasDistrict Attorney's Report On Police Shooting in Eagle PointMail Tribune100% (1)
- Subscription Suit Findings of FactDocumento127 páginasSubscription Suit Findings of FactMail TribuneAún no hay calificaciones
- Lawsuit Against Oregon State PoliceDocumento27 páginasLawsuit Against Oregon State PoliceMail TribuneAún no hay calificaciones
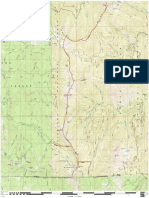
- Boundary National Recreation Trail (Klamath NF)Documento1 páginaBoundary National Recreation Trail (Klamath NF)Mail TribuneAún no hay calificaciones
- Grand Jury EP Officer Involved ShootingDocumento154 páginasGrand Jury EP Officer Involved ShootingMail TribuneAún no hay calificaciones
- Oregon Basin Outlook Report: March 2019Documento39 páginasOregon Basin Outlook Report: March 2019Mail TribuneAún no hay calificaciones
- Prospect Education Association ComplaintDocumento4 páginasProspect Education Association ComplaintMail TribuneAún no hay calificaciones
- Graves LawsuitDocumento13 páginasGraves LawsuitMail Tribune100% (1)
- Transcript of Eagle Point Police Bodycam During Officer-Involved ShootingDocumento10 páginasTranscript of Eagle Point Police Bodycam During Officer-Involved ShootingMail TribuneAún no hay calificaciones
- Boundary National Recreation Trail (RRSNF)Documento1 páginaBoundary National Recreation Trail (RRSNF)Mail TribuneAún no hay calificaciones
- Job Growth Rate Over Time Jackson County (8712)Documento1 páginaJob Growth Rate Over Time Jackson County (8712)Mail TribuneAún no hay calificaciones
- Credit risk management techniquesDocumento6 páginasCredit risk management techniquessayedrushdiAún no hay calificaciones
- Renewal notice for Mediclassic Insurance PolicyDocumento1 páginaRenewal notice for Mediclassic Insurance PolicyPradip for Fun JAún no hay calificaciones
- Lakshwiz Bazaar - Marketing Case Study Challenge.Documento3 páginasLakshwiz Bazaar - Marketing Case Study Challenge.Dushyant Singh SolankiAún no hay calificaciones
- Lesson 3Documento35 páginasLesson 3Bhon-Bhon AgcaoiliAún no hay calificaciones
- Accreditation Participation Requirement (APR) Section of The New 5th Edition Accreditation Manual - April2014 Requirements V2Documento1 páginaAccreditation Participation Requirement (APR) Section of The New 5th Edition Accreditation Manual - April2014 Requirements V2Amrish KambojAún no hay calificaciones
- InvoiceDocumento2 páginasInvoiceReza Andhitya PutraAún no hay calificaciones
- Grant of Equipment Authorization for ICOM Dual Band TransceiverDocumento1 páginaGrant of Equipment Authorization for ICOM Dual Band TransceiverFrancisco GomesAún no hay calificaciones
- Final Proj Sy2022-23 Agrigulay Corp.Documento4 páginasFinal Proj Sy2022-23 Agrigulay Corp.Jan Elaine CalderonAún no hay calificaciones
- Question Bank (Unit III & IV)Documento2 páginasQuestion Bank (Unit III & IV)Narasimhareddy MmkAún no hay calificaciones
- WW Grainger Mcmaster Carr CaseDocumento15 páginasWW Grainger Mcmaster Carr CaseAkhil Ayyakutty100% (2)
- Your Road Map To Financial Freedom 101Documento14 páginasYour Road Map To Financial Freedom 101Samuel TeddyAún no hay calificaciones
- Flash CourierDocumento19 páginasFlash Couriereaglewatch99Aún no hay calificaciones
- BhatbhateniDocumento2 páginasBhatbhateniTikendra BhandariAún no hay calificaciones
- RG - International General Version Parameter Model - V2.1Documento38 páginasRG - International General Version Parameter Model - V2.1Neo TcoAún no hay calificaciones
- Prioritizing Healthcare for All FilipinosDocumento2 páginasPrioritizing Healthcare for All FilipinosRhodjane Dela CruzAún no hay calificaciones
- About 8,440,000,000 Results (0.53 Seconds) : Test TestDocumento1 páginaAbout 8,440,000,000 Results (0.53 Seconds) : Test TestArvindAún no hay calificaciones
- Banking QuestionnaireDocumento4 páginasBanking QuestionnaireMayank KhareAún no hay calificaciones
- GSRTCDocumento1 páginaGSRTCPratik JayswalAún no hay calificaciones
- CH 1 PSC Lecture Slides Student VersionDocumento57 páginasCH 1 PSC Lecture Slides Student VersionsanjeeishereAún no hay calificaciones
- Microsoft Partner Network: Get up to $12K Monthly Azure Credit through MPN CompetenciesDocumento4 páginasMicrosoft Partner Network: Get up to $12K Monthly Azure Credit through MPN CompetenciesAkune SopoAún no hay calificaciones
- Emely B. Destreza resume accountingDocumento5 páginasEmely B. Destreza resume accountingJenny SerrocoAún no hay calificaciones
- Seasonal Materials Procurement PlanningDocumento5 páginasSeasonal Materials Procurement PlanningJaved AhmadAún no hay calificaciones
- LTE Interview Questions and Answers EricssonDocumento32 páginasLTE Interview Questions and Answers Ericssonusmanghani8257Aún no hay calificaciones
- MM 1: Display Purchase Order: Exercise Use The SAP Easy Access Menu in Order To Display A Purchase Time 10 MinDocumento10 páginasMM 1: Display Purchase Order: Exercise Use The SAP Easy Access Menu in Order To Display A Purchase Time 10 MinToño Gomez BarredaAún no hay calificaciones
- Cop 102 Course OutlineDocumento3 páginasCop 102 Course Outlinekevin muchungaAún no hay calificaciones
- Assignment (Fundamentals of Book - Keeping & Accounting)Documento25 páginasAssignment (Fundamentals of Book - Keeping & Accounting)api-370836989% (9)