También podría gustarte
- IonosphereDocumento1 páginaIonospheresarora_usAún no hay calificaciones
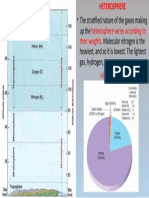
- Heterosphere: Stratified Gases by WeightDocumento1 páginaHeterosphere: Stratified Gases by Weightsarora_usAún no hay calificaciones
- World IndustriesDocumento3 páginasWorld Industriessarora_usAún no hay calificaciones
- Major Navigable CanalsDocumento18 páginasMajor Navigable Canalssarora_usAún no hay calificaciones
- Himalayan Mountain PassesDocumento1 páginaHimalayan Mountain Passessarora_usAún no hay calificaciones
- ANATOMY of A GOOD ANSWERDocumento9 páginasANATOMY of A GOOD ANSWERsarora_usAún no hay calificaciones
- Geography Mind MapDocumento1 páginaGeography Mind Mapsarora_usAún no hay calificaciones
- Structure of AtmosphereDocumento1 páginaStructure of Atmospheresarora_usAún no hay calificaciones
- Heating of AtmosphereDocumento1 páginaHeating of Atmospheresarora_usAún no hay calificaciones
- Classification of IndustriesDocumento2 páginasClassification of Industriessarora_usAún no hay calificaciones
- Building Blocks of GeographyDocumento11 páginasBuilding Blocks of Geographysarora_usAún no hay calificaciones
- Geography Optional of UPSCDocumento6 páginasGeography Optional of UPSCsarora_usAún no hay calificaciones
- Take Out Your Urban Models Chart From FridayDocumento26 páginasTake Out Your Urban Models Chart From Fridaysarora_usAún no hay calificaciones
- World Geography CanalsDocumento13 páginasWorld Geography Canalssarora_usAún no hay calificaciones
- Marine Chemistry Lecture 3Documento17 páginasMarine Chemistry Lecture 3tjsprangAún no hay calificaciones
- Bio Environment Geography Syllabus SlideDocumento6 páginasBio Environment Geography Syllabus Slidesarora_usAún no hay calificaciones
- Soil pollution: Understanding causes, effects and control measuresDocumento15 páginasSoil pollution: Understanding causes, effects and control measuresEden mollierAún no hay calificaciones
- Essay Writing For MainsDocumento20 páginasEssay Writing For Mainssarora_usAún no hay calificaciones
- InsideaTornado Infographic Final SECUREDocumento1 páginaInsideaTornado Infographic Final SECURELilianaBrillianAún no hay calificaciones
- DSE-3 - Fluvial Landforms TerracesDocumento3 páginasDSE-3 - Fluvial Landforms Terracessarora_usAún no hay calificaciones
- Erosion Control With DiagramsDocumento12 páginasErosion Control With Diagramssarora_usAún no hay calificaciones
- Concept of RegionDocumento38 páginasConcept of Regionsarora_usAún no hay calificaciones
- Protected Areas of India Vis A Vis The Six Iucn Categories (K.C.A. Arun Prasad)Documento10 páginasProtected Areas of India Vis A Vis The Six Iucn Categories (K.C.A. Arun Prasad)sarora_usAún no hay calificaciones
- WSDP Lecture Planner 2020Documento2 páginasWSDP Lecture Planner 2020sarora_usAún no hay calificaciones
- Environmental LegislationDocumento38 páginasEnvironmental Legislationsarora_usAún no hay calificaciones
- India in Figures 2018Documento37 páginasIndia in Figures 2018TELUGUPATHAMAún no hay calificaciones
- Test Series Student ReviewsDocumento1 páginaTest Series Student Reviewssarora_usAún no hay calificaciones
- Wildlife (Protection) Act, 1972Documento74 páginasWildlife (Protection) Act, 1972palatul89Aún no hay calificaciones
- Protected Areas of India Vis A Vis The Six Iucn Categories (K.C.A. Arun Prasad)Documento10 páginasProtected Areas of India Vis A Vis The Six Iucn Categories (K.C.A. Arun Prasad)sarora_usAún no hay calificaciones
- Energy Statistics 2018 PDFDocumento110 páginasEnergy Statistics 2018 PDFHemendra Kumar SainiAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- What Is Taekwondo?Documento14 páginasWhat Is Taekwondo?Josiah Salamanca SantiagoAún no hay calificaciones
- A Case Study of The Best Practices On Good Local Governance in The City of General TriasDocumento29 páginasA Case Study of The Best Practices On Good Local Governance in The City of General TriasChristina AureAún no hay calificaciones
- Business LawDocumento4 páginasBusiness LawMelissa Kayla ManiulitAún no hay calificaciones
- Mind Map All in One PBA-2021-08-20 12-38-51Documento1 páginaMind Map All in One PBA-2021-08-20 12-38-51MikosamirAún no hay calificaciones
- Intermediate Algebra For College Students 7th Edition Blitzer Test BankDocumento19 páginasIntermediate Algebra For College Students 7th Edition Blitzer Test Bankdireful.trunnionmnwf5100% (30)
- SYD611S Individual Assignment 2024Documento2 páginasSYD611S Individual Assignment 2024Amunyela FelistasAún no hay calificaciones
- La Fuerza de La Fe, de La Esperanza y El AmorDocumento2 páginasLa Fuerza de La Fe, de La Esperanza y El Amorandres diazAún no hay calificaciones
- Human Resource Management: Functions and ObjectivesDocumento26 páginasHuman Resource Management: Functions and ObjectivesABDUL RAZIQ REHANAún no hay calificaciones
- Gender, Race, and Semicolonialism: Liu Na'ou's Urban Shanghai LandscapeDocumento24 páginasGender, Race, and Semicolonialism: Liu Na'ou's Urban Shanghai Landscapebaiqian liuAún no hay calificaciones
- EXL ServiceDocumento2 páginasEXL ServiceMohit MishraAún no hay calificaciones
- Aclc College of Tacloban Tacloban CityDocumento3 páginasAclc College of Tacloban Tacloban Cityjumel delunaAún no hay calificaciones
- Chua v. CFI DigestDocumento1 páginaChua v. CFI DigestMae Ann Sarte AchaAún no hay calificaciones
- Esmf 04052017 PDFDocumento265 páginasEsmf 04052017 PDFRaju ReddyAún no hay calificaciones
- Cristina Gallardo CV - English - WebDocumento2 páginasCristina Gallardo CV - English - Webcgallardo88Aún no hay calificaciones
- Wa0010Documento3 páginasWa0010BRANDO LEONARDO ROJAS ROMEROAún no hay calificaciones
- SECTION 26. Registration of Threatened and Exotic Wildlife in The Possession of Private Persons. - NoDocumento5 páginasSECTION 26. Registration of Threatened and Exotic Wildlife in The Possession of Private Persons. - NoAron PanturillaAún no hay calificaciones
- RAS MARKAZ CRUDE OIL PARK SITE INSPECTION PROCEDUREDocumento1 páginaRAS MARKAZ CRUDE OIL PARK SITE INSPECTION PROCEDUREANIL PLAMOOTTILAún no hay calificaciones
- History, and Culture of DenmarkDocumento14 páginasHistory, and Culture of DenmarkRina ApriliaAún no hay calificaciones
- ePass for Essential Travel Between Andhra Pradesh and OdishaDocumento1 páginaePass for Essential Travel Between Andhra Pradesh and OdishaganeshAún no hay calificaciones
- Guidelines: For Submitting A Candidature To OrganiseDocumento19 páginasGuidelines: For Submitting A Candidature To OrganiseDan ZoltnerAún no hay calificaciones
- 1 292583745 Bill For Current Month 1Documento2 páginas1 292583745 Bill For Current Month 1Shrotriya AnamikaAún no hay calificaciones
- Notice WritingDocumento2 páginasNotice WritingMeghana ChaudhariAún no hay calificaciones
- Mid-Term Quiz Sample AnswersDocumento4 páginasMid-Term Quiz Sample AnswersNamAún no hay calificaciones
- Sohan vs. Mohan PlaintDocumento6 páginasSohan vs. Mohan PlaintKarandeep Saund100% (5)
- Chapter 1 Capstone Case: New Century Wellness GroupDocumento4 páginasChapter 1 Capstone Case: New Century Wellness GroupJC100% (7)
- DIN EN ISO 12944-4 071998-EnDocumento29 páginasDIN EN ISO 12944-4 071998-EnChristopher MendozaAún no hay calificaciones
- Pudri RekpungDocumento1 páginaPudri Rekpungpz.pzzzzAún no hay calificaciones
- Cruise LetterDocumento23 páginasCruise LetterSimon AlvarezAún no hay calificaciones
- 2024 JanuaryDocumento9 páginas2024 Januaryedgardo61taurusAún no hay calificaciones
- Encyclopædia Americana - Vol II PDFDocumento620 páginasEncyclopædia Americana - Vol II PDFRodrigo SilvaAún no hay calificaciones