También podría gustarte
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Urology MCQs For Posgraduate Exam PDFDocumento62 páginasUrology MCQs For Posgraduate Exam PDFsiddavaram srideep100% (1)
- Pathophysiology Diagram of Congestive Heart FailureDocumento3 páginasPathophysiology Diagram of Congestive Heart Failurea_samiane64% (11)
- Cardiolog Y: Dian Paramita Kartikasari MAY, 17THDocumento51 páginasCardiolog Y: Dian Paramita Kartikasari MAY, 17THDian ParamitaAún no hay calificaciones
- 9autacoids 14010v9023022 Phpapp02Documento109 páginas9autacoids 14010v9023022 Phpapp02h3cn1r3100% (1)
- USMLE WORLD QUESTIONS QuizletDocumento87 páginasUSMLE WORLD QUESTIONS QuizletPatricio AlexanderAún no hay calificaciones
- Mishba +pharmacology + Tapan ShahDocumento232 páginasMishba +pharmacology + Tapan ShahRaushan BlakeAún no hay calificaciones
- HYPERALDOSTERONISMDocumento7 páginasHYPERALDOSTERONISMMarnee Justine ColladoAún no hay calificaciones
- Kamus AnatomiDocumento42 páginasKamus AnatomiAbdul Al-hadiAún no hay calificaciones
- Pathophysiology of Acute Renal FailureDocumento2 páginasPathophysiology of Acute Renal Failureminangsung minangnengAún no hay calificaciones
- Final Physiology... Medical 2Documento12 páginasFinal Physiology... Medical 2Ishaq DerbashiAún no hay calificaciones
- Mindanao State University - Iligan Institute of Technology Student: - SectionDocumento2 páginasMindanao State University - Iligan Institute of Technology Student: - SectionJohn Pearl FernandezAún no hay calificaciones
- Surgery - PPT'sDocumento172 páginasSurgery - PPT'sShreya KulkarniAún no hay calificaciones
- Biochem Lec Notes For ReadingDocumento51 páginasBiochem Lec Notes For ReadingShaira Elyze GabrielAún no hay calificaciones
- HYPERTENSION CASE MANAGEMENTDocumento49 páginasHYPERTENSION CASE MANAGEMENTCarl Angelo SuaybaguioAún no hay calificaciones
- Chapter 6 Body Fluids, Water-Salt and Acid-Base BalanceDocumento69 páginasChapter 6 Body Fluids, Water-Salt and Acid-Base Balancefatin harrisAún no hay calificaciones
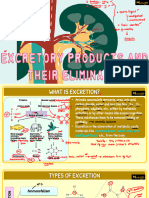
- Vipin Sir Biology 19. Excretory Products and Their EliminationDocumento55 páginasVipin Sir Biology 19. Excretory Products and Their EliminationvanshpatelssisAún no hay calificaciones
- Adrenal Function: T. Creighton Mitchell, A. Wayne MeikleDocumento19 páginasAdrenal Function: T. Creighton Mitchell, A. Wayne MeikleWho KnowsAún no hay calificaciones
- Renal System Functions and DisordersDocumento4 páginasRenal System Functions and DisordersLordgelyn Diane ViernesAún no hay calificaciones
- Quizlet Test 10 CHP 50,51,52Documento7 páginasQuizlet Test 10 CHP 50,51,52Jacqueline GreerAún no hay calificaciones
- Types of ShocksDocumento33 páginasTypes of Shocksmark OrpillaAún no hay calificaciones
- Pathophysiology and Etiology of Edema in AdultsDocumento15 páginasPathophysiology and Etiology of Edema in AdultsJovie Anne CabangalAún no hay calificaciones
- Study Questions Urinary SystemDocumento32 páginasStudy Questions Urinary Systemandy_jean_2100% (1)
- Saltwater Power: Samal National High SchoolDocumento47 páginasSaltwater Power: Samal National High SchoolKhloe EppohsAún no hay calificaciones
- ACE Inhibitors Vs ARBsDocumento3 páginasACE Inhibitors Vs ARBsKo Phyo WaiAún no hay calificaciones
- Fluid and Electrolyte Balance LectureDocumento16 páginasFluid and Electrolyte Balance LectureBasa, Rica Mae P.Aún no hay calificaciones
- 19-Year-Old Female With Hypokalemia EvaluatedDocumento5 páginas19-Year-Old Female With Hypokalemia EvaluatedMohammed AhmedAún no hay calificaciones
- Renal Embryology: Jason Ryan, MD, MPHDocumento731 páginasRenal Embryology: Jason Ryan, MD, MPHFateh BoulounisAún no hay calificaciones
- Tmp1a96 TMPDocumento80 páginasTmp1a96 TMPFrontiersAún no hay calificaciones
- Sodium and Water Need To KnowDocumento48 páginasSodium and Water Need To KnowkartikaparamitaAún no hay calificaciones
- Regulation of ElectrolytesDocumento28 páginasRegulation of ElectrolytesnirilibAún no hay calificaciones