También podría gustarte
- Star WarsDocumento1 páginaStar WarsVinicius Fernandes AraujoAún no hay calificaciones
- Ran - Piano (Feat. Andi Rianto)Documento1 páginaRan - Piano (Feat. Andi Rianto)IkrarAbdillahAún no hay calificaciones
- Prostate and Seminal VesiclesDocumento3 páginasProstate and Seminal VesiclesIkrarAbdillahAún no hay calificaciones
- Progress NoteDocumento7 páginasProgress NoteIkrarAbdillahAún no hay calificaciones
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- PGDPM S1 Module 2 TestDocumento5 páginasPGDPM S1 Module 2 TestLevi MuromboAún no hay calificaciones
- Muslim Women in The Tenement Gardens of Colombo: A Story of Marginalization, Legitimized by A Culture of OppressionDocumento36 páginasMuslim Women in The Tenement Gardens of Colombo: A Story of Marginalization, Legitimized by A Culture of OppressionSocial Scientists' AssociationAún no hay calificaciones
- Wilkinson Rogers Formula 2346786Documento9 páginasWilkinson Rogers Formula 2346786Raja SooriamurthiAún no hay calificaciones
- Leveraging Consumer Behavior: How Coca-Cola Targets the Indian MarketDocumento12 páginasLeveraging Consumer Behavior: How Coca-Cola Targets the Indian MarketKarthikeyan ThiagarajanAún no hay calificaciones
- Questioning Minds: Yung-Hee KimDocumento250 páginasQuestioning Minds: Yung-Hee Kim김새증Aún no hay calificaciones
- Admin Law Prefinal NotesDocumento14 páginasAdmin Law Prefinal NotesSanson OrozcoAún no hay calificaciones
- Affidavit of Non Tenancy Rosalina LiaoDocumento2 páginasAffidavit of Non Tenancy Rosalina LiaoEppie SeverinoAún no hay calificaciones
- FIN Act 2 - OdysseyDocumento2 páginasFIN Act 2 - OdysseyJanwyne NgAún no hay calificaciones
- Reflection Paper About Locomotor and Non-Locomotor MovementsDocumento1 páginaReflection Paper About Locomotor and Non-Locomotor MovementsanaryAún no hay calificaciones
- The Province of North Cotabato, Et Al - V - The Government of The Republic of The Philippines, Et Al .Documento11 páginasThe Province of North Cotabato, Et Al - V - The Government of The Republic of The Philippines, Et Al .Arbee ArquizaAún no hay calificaciones
- MBR-Mobile Banking Research Proposal - OmaidDocumento13 páginasMBR-Mobile Banking Research Proposal - OmaidOmaid100% (1)
- Internal Communication Assignment - Communicating Strategy: Starting PointDocumento4 páginasInternal Communication Assignment - Communicating Strategy: Starting PointNiaAún no hay calificaciones
- Application Letter and ResumeDocumento2 páginasApplication Letter and ResumeLindon Jay EnclunaAún no hay calificaciones
- Hunter Reference SheetDocumento2 páginasHunter Reference SheetPolly CampbellAún no hay calificaciones
- Symmetrical Triangles - Chart Formations That Consolidate Before BreakoutsDocumento13 páginasSymmetrical Triangles - Chart Formations That Consolidate Before BreakoutsYin Shen Goh100% (4)
- CHAPTER VI CREATING BRAND EQUITY - Manansala - RolynDocumento16 páginasCHAPTER VI CREATING BRAND EQUITY - Manansala - RolynROLYNAún no hay calificaciones
- Termination and Adoption PetitionDocumento4 páginasTermination and Adoption Petitionjuakin12350% (4)
- Ryanair Case Study AnalysisDocumento5 páginasRyanair Case Study Analysisbinzidd00767% (3)
- Rathore - Political SociologyDocumento23 páginasRathore - Political SociologyCybs BiasbasAún no hay calificaciones
- Julian RzoskaDocumento409 páginasJulian RzoskaPietro FuscoAún no hay calificaciones
- A Study On The Attitude of B.ed Students Towards Computer EducationDocumento8 páginasA Study On The Attitude of B.ed Students Towards Computer EducationAnonymous CwJeBCAXpAún no hay calificaciones
- Day 3 Las - Ratio and ProportionDocumento7 páginasDay 3 Las - Ratio and ProportionPrecious Joy Torayno BayawaAún no hay calificaciones
- RECTO MEMORIAL NATIONAL HIGH SCHOOL Social Sciences ProfessionsDocumento11 páginasRECTO MEMORIAL NATIONAL HIGH SCHOOL Social Sciences ProfessionsVince BurceAún no hay calificaciones
- Management Unit 4 4 3 Evaluate The Manager As A Leader 2015Documento4 páginasManagement Unit 4 4 3 Evaluate The Manager As A Leader 2015api-312882401Aún no hay calificaciones
- Powerpoint Presentation 3.1Documento19 páginasPowerpoint Presentation 3.1Jack PennAún no hay calificaciones
- Unit 2 - 1Documento19 páginasUnit 2 - 1dollyAún no hay calificaciones
- NAtural LogarithmDocumento15 páginasNAtural Logarithmjohn tanAún no hay calificaciones
- Case BriefDocumento5 páginasCase BriefEs-EsAún no hay calificaciones
- BOT330 SyllabusDocumento10 páginasBOT330 SyllabusvinsletsoinAún no hay calificaciones
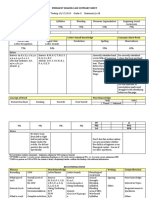
- Emergent Reader Case Summary SheetDocumento2 páginasEmergent Reader Case Summary Sheetapi-503192153Aún no hay calificaciones