También podría gustarte
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- A-Z Romantic WordsDocumento7 páginasA-Z Romantic Wordsjoshsande100% (4)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2101)
- SuccubusDocumento2 páginasSuccubuspauljonesgarciaAún no hay calificaciones
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Fundamentals of Treatment PlanningDocumento310 páginasFundamentals of Treatment PlanningLekic Jelena100% (4)
- Women in MedicineDocumento280 páginasWomen in MedicineLekic JelenaAún no hay calificaciones
- WWW Passionescorts NetDocumento12 páginasWWW Passionescorts NetBangalore EscortsAún no hay calificaciones
- Dejection An OdeDocumento6 páginasDejection An Odeanjumdk75% (4)
- Principles of Floral DesignDocumento22 páginasPrinciples of Floral DesignKarol Ionas100% (5)
- Lanza Product Reference GuideDocumento64 páginasLanza Product Reference GuideEdwardAún no hay calificaciones
- CAD CAM DigitalImpressions Website1Documento11 páginasCAD CAM DigitalImpressions Website1fzroshani100% (1)
- CAD CAM DigitalImpressions Website1Documento11 páginasCAD CAM DigitalImpressions Website1fzroshani100% (1)
- Canadian Researcher Dr. Joanne Wood and Her Team at The University of Waterloo Published A Study in The (That Says, "Documento2 páginasCanadian Researcher Dr. Joanne Wood and Her Team at The University of Waterloo Published A Study in The (That Says, "Shravya ShrutiAún no hay calificaciones
- Conditioner FormulasDocumento4 páginasConditioner FormulasCarolina TarifAún no hay calificaciones
- What Does The Word Beauty Mean To YouDocumento1 páginaWhat Does The Word Beauty Mean To YouPillos Jr., Elimar0% (1)
- CatioLift Technical InformationDocumento9 páginasCatioLift Technical InformationNazihCosmetics0% (1)
- Undetectable Hair Transplants by Dr. Ch. Krishna PriyaDocumento155 páginasUndetectable Hair Transplants by Dr. Ch. Krishna PriyaKrishna RayaluAún no hay calificaciones
- Chekhov EssayDocumento137 páginasChekhov EssayocchityaAún no hay calificaciones
- Oralni Tus KatalogDocumento6 páginasOralni Tus KatalogLekic JelenaAún no hay calificaciones
- Art TherapyDocumento420 páginasArt TherapyLekic Jelena29% (21)
- The Adhesive Bridge Inlay Retained in The TherapyDocumento3 páginasThe Adhesive Bridge Inlay Retained in The TherapyLekic JelenaAún no hay calificaciones
- Cadcam Systems MaterialsDocumento9 páginasCadcam Systems MaterialsCorina BolatAún no hay calificaciones
- Computer-Aided Design and Computer-Assisted Manufacturing in Prosthetic Implant DentistryDocumento8 páginasComputer-Aided Design and Computer-Assisted Manufacturing in Prosthetic Implant DentistryLekic JelenaAún no hay calificaciones
- Aesthetics N' VeneersDocumento7 páginasAesthetics N' VeneersmusaabsiddiquiAún no hay calificaciones
- JADA 2006 Christensen 661 4Documento4 páginasJADA 2006 Christensen 661 4Lekic JelenaAún no hay calificaciones
- JADA 2011 Edelhoff 14S 9SDocumento7 páginasJADA 2011 Edelhoff 14S 9SLekic JelenaAún no hay calificaciones
- Laboratory IBERPRECISDocumento6 páginasLaboratory IBERPRECISLekic JelenaAún no hay calificaciones
- Abstract Ind CT EnglDocumento3 páginasAbstract Ind CT EnglLekic JelenaAún no hay calificaciones
- 14Documento6 páginas14Lekic JelenaAún no hay calificaciones
- (Contemporary Japan) Kiyoku Tadashiku Utsukushiku Takarazuka Revue and The Project of Identity (Re-) SolidificationDocumento21 páginas(Contemporary Japan) Kiyoku Tadashiku Utsukushiku Takarazuka Revue and The Project of Identity (Re-) SolidificationLucía AlbarracinAún no hay calificaciones
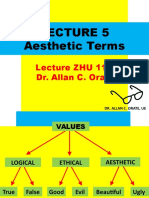
- Prof. Orate Lecture 5Documento27 páginasProf. Orate Lecture 5jihoonie67100% (1)
- 4akid Catalogue 2 - Clothing & Accessories PDFDocumento27 páginas4akid Catalogue 2 - Clothing & Accessories PDFRamon Harvey0% (1)
- 50 Most Common Proverbs - Print de 2 OriDocumento5 páginas50 Most Common Proverbs - Print de 2 OriIoanaR2011Aún no hay calificaciones
- Gilman, Sander L. - Black Bodies, White BodiesDocumento40 páginasGilman, Sander L. - Black Bodies, White BodiesAndi TothAún no hay calificaciones
- Elegy (2008) : Directed By: Based On The Novel byDocumento4 páginasElegy (2008) : Directed By: Based On The Novel byapi-212891764Aún no hay calificaciones
- Black RookDocumento16 páginasBlack Rookapi-236470498Aún no hay calificaciones
- Star Yarn - Art ClassDocumento5 páginasStar Yarn - Art ClassAngela ReyesAún no hay calificaciones
- How Beauty Standards Came To BeDocumento3 páginasHow Beauty Standards Came To Beapi-537797933Aún no hay calificaciones
- Aak-Lfc Lipex Shea Betaine 0808Documento2 páginasAak-Lfc Lipex Shea Betaine 0808icraoAún no hay calificaciones
- Legend of SampaguitaDocumento4 páginasLegend of SampaguitaAndreiFoxAún no hay calificaciones
- Hymn To RaDocumento3 páginasHymn To Radancinggoat23100% (1)
- Geography: The Idea For The Modern Philippine Flag's Design Came in 1897 From General Emilio AguinaldoDocumento5 páginasGeography: The Idea For The Modern Philippine Flag's Design Came in 1897 From General Emilio AguinaldoShynne AbadianoAún no hay calificaciones
- Product Research - ShampooDocumento16 páginasProduct Research - ShampooraguldrdAún no hay calificaciones
- PG English PDFDocumento33 páginasPG English PDFAbhisek RoyBarmanAún no hay calificaciones
- Revised ScriptDocumento16 páginasRevised ScriptLei Andre LlandaAún no hay calificaciones
- PC 1118 PDFDocumento2 páginasPC 1118 PDFrafaeldelperu1982Aún no hay calificaciones
- Review Text Movie The Story of MaleficentDocumento3 páginasReview Text Movie The Story of Maleficentberliana putriAún no hay calificaciones