También podría gustarte
- ACOG Management of Stillbirth PDFDocumento14 páginasACOG Management of Stillbirth PDFLêMinhĐứcAún no hay calificaciones
- Intrauterine Growth RestrictionDocumento7 páginasIntrauterine Growth RestrictionNurfazlinaAún no hay calificaciones
- Handbook of Current and Novel Protocols for the Treatment of InfertilityDe EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanAún no hay calificaciones
- Recurrent MiscarriageDocumento6 páginasRecurrent MiscarriageuzmajbnAún no hay calificaciones
- PROLOG: Patient Management in the Office, Eighth EditionDe EverandPROLOG: Patient Management in the Office, Eighth EditionAún no hay calificaciones
- Ultrasound Fundamentals An Evidence Based Guide For Medical PractitionersDocumento372 páginasUltrasound Fundamentals An Evidence Based Guide For Medical Practitionersahmet kutluayAún no hay calificaciones
- Induction of Labor With Oxytocin - UpToDateDocumento54 páginasInduction of Labor With Oxytocin - UpToDateJhoseline CamposAún no hay calificaciones
- Occiput Posterior Position Diagnosis VagDocumento19 páginasOcciput Posterior Position Diagnosis VagMutianaUmminyaKhanzaAún no hay calificaciones
- FIGO Accreta Prenantal DiagnosisDocumento7 páginasFIGO Accreta Prenantal DiagnosisYosef Dwi Cahyadi SalanAún no hay calificaciones
- Bad Obstetrical HistoryDocumento34 páginasBad Obstetrical HistorySagung Ayuska GandhariAún no hay calificaciones
- Implantation and Development Placenta Part 2Documento36 páginasImplantation and Development Placenta Part 2Tengku Chairannisa PutriAún no hay calificaciones
- Recurrent Pregnancy LossDocumento19 páginasRecurrent Pregnancy LossSean NamAún no hay calificaciones
- (SLE) and PregnancyDocumento39 páginas(SLE) and PregnancyRake SardevaAún no hay calificaciones
- Cardiac Disease and Pregnancy RCOG GuidelineDocumento18 páginasCardiac Disease and Pregnancy RCOG GuidelinedanielsusenoAún no hay calificaciones
- Ultrasound Diagnosis of Early Pregnancy LossDocumento18 páginasUltrasound Diagnosis of Early Pregnancy LossxxdrivexxAún no hay calificaciones
- Rcog PpromDocumento7 páginasRcog PpromDevi SyamAún no hay calificaciones
- ACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Documento15 páginasACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Reza ZulkarnainAún no hay calificaciones
- Amnioinfusion - LEODocumento16 páginasAmnioinfusion - LEOtapayanaAún no hay calificaciones
- Overview Antenatal CareDocumento54 páginasOverview Antenatal CareRizky Dwidya AmirtasariAún no hay calificaciones
- (SLE) and PregnancyDocumento60 páginas(SLE) and PregnancyNurfikhaHandayaniAún no hay calificaciones
- Misoprostol Dosage Recommendations 2012 4Documento1 páginaMisoprostol Dosage Recommendations 2012 4Bonifacius Bayu Erlangga KusumaAún no hay calificaciones
- Abnormal Uterine Bleeding: District 1 ACOG Medical Student Education Module 2008Documento17 páginasAbnormal Uterine Bleeding: District 1 ACOG Medical Student Education Module 2008ninachayank0% (1)
- Sarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalDocumento2 páginasSarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalTan Chin AunAún no hay calificaciones
- Adrianes Bachnas - Preeclampsia Screening Algorythm 2Documento23 páginasAdrianes Bachnas - Preeclampsia Screening Algorythm 2Wienda GeraldineAún no hay calificaciones
- Skor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermDocumento9 páginasSkor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermMuhammad KhoiruddinAún no hay calificaciones
- Ostpartum Hemorrhage: Dr. Patiyus Agustiansyah, Spog (K)Documento70 páginasOstpartum Hemorrhage: Dr. Patiyus Agustiansyah, Spog (K)JoAún no hay calificaciones
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDocumento7 páginasEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloAún no hay calificaciones
- RPL DR KanadiDocumento26 páginasRPL DR KanadiParvaAún no hay calificaciones
- Printable - Thesis On Bishop ScoreDocumento103 páginasPrintable - Thesis On Bishop Scoreanuaurv100% (3)
- Acog Vbac PDFDocumento14 páginasAcog Vbac PDFFrancyn Rossi YangsonAún no hay calificaciones
- Judi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009Documento66 páginasJudi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009emilyakmanAún no hay calificaciones
- Amniotic Fluid Index (AFI)Documento1 páginaAmniotic Fluid Index (AFI)dgina8800100% (1)
- Ob-Gyn (Clinic/Office) Nurse: OB/GYN Nurses Provide A Variety of Functions Related To The Female Reproductive SystemDocumento13 páginasOb-Gyn (Clinic/Office) Nurse: OB/GYN Nurses Provide A Variety of Functions Related To The Female Reproductive SystemJaclyn SarmientoAún no hay calificaciones
- Induction of Labor: Nor Fareshah BT Mohd Nasir 071303057 Batch 21/ F2Documento47 páginasInduction of Labor: Nor Fareshah BT Mohd Nasir 071303057 Batch 21/ F2Nor Fareshah100% (1)
- ACOG 2009 Induction of LaborDocumento12 páginasACOG 2009 Induction of LaborRiantiara PutrizaAún no hay calificaciones
- Multifetal PregnancyDocumento11 páginasMultifetal PregnancyDr. ZeekAún no hay calificaciones
- Male InfertilityDocumento63 páginasMale InfertilitySuhaila SabanAún no hay calificaciones
- Tugas SC Vs Histerotomi Vs Laparotomi Ambil Anak Aji PatriajatiDocumento3 páginasTugas SC Vs Histerotomi Vs Laparotomi Ambil Anak Aji PatriajatiAji PatriajatiAún no hay calificaciones
- Operative Vaginal Delivery PDFDocumento56 páginasOperative Vaginal Delivery PDFFarehan Md IsaAún no hay calificaciones
- ACOG-49 Dystocia and Augmentation of LaborDocumento10 páginasACOG-49 Dystocia and Augmentation of LaborAngeredYetiAún no hay calificaciones
- Jadwal Pit (Fetomaternal Room)Documento3 páginasJadwal Pit (Fetomaternal Room)Dwi Adi NugrohoAún no hay calificaciones
- Mnemonic Vacum Dan Forcep NewDocumento2 páginasMnemonic Vacum Dan Forcep NewsinggehAún no hay calificaciones
- Ectopic PregnancyDocumento24 páginasEctopic PregnancybertouwAún no hay calificaciones
- 3 16Documento27 páginas3 16Iful SaifullahAún no hay calificaciones
- Review Adnexal Masses Pregnancy Rcog PDFDocumento6 páginasReview Adnexal Masses Pregnancy Rcog PDFRosália Coutada100% (1)
- Gestational Trophoblastic DiseasesDocumento37 páginasGestational Trophoblastic DiseasesEdwin OkonAún no hay calificaciones
- Abortion PresentationDocumento46 páginasAbortion PresentationJhong Xyrus67% (3)
- Practice Bulletin: Management of Preterm LaborDocumento10 páginasPractice Bulletin: Management of Preterm LaborXimena OrtegaAún no hay calificaciones
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocumento9 páginasEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyfujimeisterAún no hay calificaciones
- Myop in PregnancyDocumento4 páginasMyop in PregnancySamuel WilliamsAún no hay calificaciones
- Acute Abdomen During Pregnancy BelaynehDocumento47 páginasAcute Abdomen During Pregnancy BelaynehYohannis AsefaAún no hay calificaciones
- AmenorrheaDocumento56 páginasAmenorrheaMrTriumphantAún no hay calificaciones
- Reproductive Endocrinology FinalDocumento98 páginasReproductive Endocrinology FinalChino Paolo SamsonAún no hay calificaciones
- FK UNS OBGIN USG 1i. Skrining Anomali Trimester Dua ISUOG Guidelines JJE 20120609Documento66 páginasFK UNS OBGIN USG 1i. Skrining Anomali Trimester Dua ISUOG Guidelines JJE 20120609Judi Januadi Endjun, MD, ObsGyn100% (1)
- Bunt - Male and Female Infertility USAFP 2009-v2 (PPTminimizer)Documento35 páginasBunt - Male and Female Infertility USAFP 2009-v2 (PPTminimizer)Jalajarani AridassAún no hay calificaciones
- Unas Mei 2020 (Sule) : Yang Dianggap Soal BaruDocumento15 páginasUnas Mei 2020 (Sule) : Yang Dianggap Soal Baruhari ilman toniAún no hay calificaciones
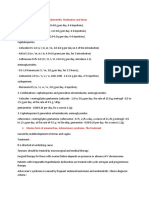
- Treatment of Acute Endometritis. Medication and DosesDocumento3 páginasTreatment of Acute Endometritis. Medication and DosesTitoun LettounAún no hay calificaciones
- AUB Current Update (Malam Keakraban PAOGI)Documento36 páginasAUB Current Update (Malam Keakraban PAOGI)armillaraissyaAún no hay calificaciones
- Opioid and Benzodiazepine Weaning in Pediatric PatientsDocumento25 páginasOpioid and Benzodiazepine Weaning in Pediatric PatientsMaverick 18Aún no hay calificaciones
- Powertemplate: ThemegalleryDocumento30 páginasPowertemplate: ThemegalleryMaverick 18Aún no hay calificaciones
- Utility of Neurodiagnostic Studies in The Diagnosis of Autoimmune Encephalitis in PDFDocumento26 páginasUtility of Neurodiagnostic Studies in The Diagnosis of Autoimmune Encephalitis in PDFMaverick 18Aún no hay calificaciones
- Medicina InternaDocumento693 páginasMedicina InternaMaverick 18100% (5)
- Wildlife Carving in Relief Carving Techniques and Patterns PDFDocumento173 páginasWildlife Carving in Relief Carving Techniques and Patterns PDFMaverick 18100% (4)
- Practice Bulletin No. 135 - Second-Trimester Abortion.Documento13 páginasPractice Bulletin No. 135 - Second-Trimester Abortion.Maverick 18Aún no hay calificaciones
- Practice Bulletins No. 139 - Premature Rupture of Membranes.Documento13 páginasPractice Bulletins No. 139 - Premature Rupture of Membranes.Maverick 18100% (1)
- Relation Between Obesity and Bone Mineral Density and Vertebral Fractures in Korean Postmenopausal WomenDocumento7 páginasRelation Between Obesity and Bone Mineral Density and Vertebral Fractures in Korean Postmenopausal WomenMaverick 18Aún no hay calificaciones
- Code of Ethics: Registered Beauty TherapistsDocumento9 páginasCode of Ethics: Registered Beauty Therapistssilvia oanaAún no hay calificaciones
- Racap Covid-19 Map InsightsDocumento9 páginasRacap Covid-19 Map Insightsbrowry manaluAún no hay calificaciones
- Csbpr7 Acute Stroke Management Module Final Eng 2022Documento161 páginasCsbpr7 Acute Stroke Management Module Final Eng 2022Vigneshwara NagarajanAún no hay calificaciones
- Health and Wellness: Distinguishing Screening, Evaluation and ExaminationDocumento14 páginasHealth and Wellness: Distinguishing Screening, Evaluation and ExaminationsaddaqatAún no hay calificaciones
- June 2015 Paper 1-15-16 NCSEDocumento2 páginasJune 2015 Paper 1-15-16 NCSERiah TiffanyAún no hay calificaciones
- Attending Physician Name: Medical Information Sheet - Medif - Part 2Documento1 páginaAttending Physician Name: Medical Information Sheet - Medif - Part 2San Ban CastroAún no hay calificaciones
- Studycovidspread, Severityin Children, Young:PmtoofficialsDocumento16 páginasStudycovidspread, Severityin Children, Young:PmtoofficialsshivamAún no hay calificaciones
- Exercise and Mental HealthDocumento3 páginasExercise and Mental HealthMelat Assegid100% (1)
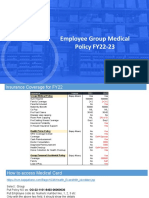
- Employee Group Medical Policy FY22-23: Merchant ExperienceDocumento7 páginasEmployee Group Medical Policy FY22-23: Merchant ExperienceLokesh SharmaAún no hay calificaciones
- ANNEX 9 Project Work Plan and Budget MatrixDocumento2 páginasANNEX 9 Project Work Plan and Budget MatrixSharifa Aynee JamsuriAún no hay calificaciones
- Btech Companies ListDocumento5 páginasBtech Companies ListArslan AliAún no hay calificaciones
- Lesson 1 Concepts of Comunity Environmental Health Wk1 1Documento28 páginasLesson 1 Concepts of Comunity Environmental Health Wk1 1jckydeleonAún no hay calificaciones
- Denture Esthetics: There Is More Than Teeth Replacement: September 2014Documento4 páginasDenture Esthetics: There Is More Than Teeth Replacement: September 2014Krupali JainAún no hay calificaciones
- C Ovid 19 Positive Test Report FormDocumento2 páginasC Ovid 19 Positive Test Report FormMinaketan DasAún no hay calificaciones
- jpsr09021729 PDFDocumento6 páginasjpsr09021729 PDFirsyad tsaniAún no hay calificaciones
- Ra-114510 Criminologist Tuguegarao 6-2022Documento146 páginasRa-114510 Criminologist Tuguegarao 6-2022G2-Peter Paul PacionAún no hay calificaciones
- Ch-1 PC4 History of Public Health NursingDocumento23 páginasCh-1 PC4 History of Public Health Nursingmaha abdallahAún no hay calificaciones
- Children 09 00731Documento16 páginasChildren 09 00731vikaAún no hay calificaciones
- Inpatient Handbook 2008-2009 UCLADocumento275 páginasInpatient Handbook 2008-2009 UCLAartig44Aún no hay calificaciones
- NCM 107 Worksheet Week 16.v2Documento2 páginasNCM 107 Worksheet Week 16.v2Andrei BorataAún no hay calificaciones
- Dorothea Orem Theory AnalysisDocumento2 páginasDorothea Orem Theory AnalysisKara Kristine Tuano NarismaAún no hay calificaciones
- Preliminary Programme ERC2011Documento12 páginasPreliminary Programme ERC2011ExpuneriMedicaleAún no hay calificaciones
- Aro Village SystemDocumento5 páginasAro Village SystemObehi EromoseleAún no hay calificaciones
- Acupuncture For Chronic PainDocumento9 páginasAcupuncture For Chronic PainmichAún no hay calificaciones
- Filippo Cardinali Fabio Gorni: The Use of The Rubber Dam in EndodonticsDocumento78 páginasFilippo Cardinali Fabio Gorni: The Use of The Rubber Dam in EndodonticsMara Bejnariu100% (1)
- Begs 183Documento4 páginasBegs 183viploveAún no hay calificaciones
- Burns Protocol PDFDocumento18 páginasBurns Protocol PDFSai MaryAún no hay calificaciones
- Annual Product Quality Review (APQR - APR - PQR) in Quality Improvements - PharmaguidelineDocumento1 páginaAnnual Product Quality Review (APQR - APR - PQR) in Quality Improvements - Pharmaguidelinenataarajan praveenAún no hay calificaciones
- Kimberly Cremerius: ObjectiveDocumento3 páginasKimberly Cremerius: Objectiveapi-252001755Aún no hay calificaciones
- Ae Productos FarmaceuticosDocumento37 páginasAe Productos Farmaceuticosjose ricardo cisneros espinozaAún no hay calificaciones
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Calificación: 3 de 5 estrellas3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDCalificación: 5 de 5 estrellas5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionCalificación: 4 de 5 estrellas4/5 (404)
- The Comfort of Crows: A Backyard YearDe EverandThe Comfort of Crows: A Backyard YearCalificación: 4.5 de 5 estrellas4.5/5 (23)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsCalificación: 4 de 5 estrellas4/5 (4)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedCalificación: 4.5 de 5 estrellas4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityCalificación: 4 de 5 estrellas4/5 (35)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryCalificación: 4 de 5 estrellas4/5 (46)
- The Obesity Code: Unlocking the Secrets of Weight LossDe EverandThe Obesity Code: Unlocking the Secrets of Weight LossCalificación: 4 de 5 estrellas4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAún no hay calificaciones
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeCalificación: 2 de 5 estrellas2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsCalificación: 4.5 de 5 estrellas4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsCalificación: 5 de 5 estrellas5/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeDe EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeCalificación: 4.5 de 5 estrellas4.5/5 (2)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDe EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesCalificación: 4.5 de 5 estrellas4.5/5 (1412)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisCalificación: 4.5 de 5 estrellas4.5/5 (44)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDe EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisCalificación: 5 de 5 estrellas5/5 (8)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Calificación: 4.5 de 5 estrellas4.5/5 (110)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingDe EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingCalificación: 1 de 5 estrellas1/5 (2)
- To Explain the World: The Discovery of Modern ScienceDe EverandTo Explain the World: The Discovery of Modern ScienceCalificación: 3.5 de 5 estrellas3.5/5 (51)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!De EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Calificación: 5 de 5 estrellas5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDe EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsAún no hay calificaciones
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDe EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsCalificación: 4.5 de 5 estrellas4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeCalificación: 4.5 de 5 estrellas4.5/5 (254)