También podría gustarte
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Legal Medicine (Medical Jurisprudence To A Law Student)Documento14 páginasLegal Medicine (Medical Jurisprudence To A Law Student)Look ArtAún no hay calificaciones
- Building An Organization Capable of Good Strategy Execution: People, Capabilities, and StructureDocumento31 páginasBuilding An Organization Capable of Good Strategy Execution: People, Capabilities, and Structuremrt8888100% (1)
- Encyclopedia of South AfricaDocumento11 páginasEncyclopedia of South AfricaLittleWhiteBakkie100% (1)
- Business Free Talk Lesson 5Documento9 páginasBusiness Free Talk Lesson 5McJay CharitoAún no hay calificaciones
- 2 Page ResumeDocumento2 páginas2 Page ResumeRocky Hossain0% (1)
- 20170927-Ap3391 Vol3 Lflt205 Education Annex C-UDocumento8 páginas20170927-Ap3391 Vol3 Lflt205 Education Annex C-URiannab15Aún no hay calificaciones
- Refined SPJ Filipino 4 10 PamamahayagDocumento69 páginasRefined SPJ Filipino 4 10 PamamahayagCherica casinoAún no hay calificaciones
- Fred Factor TeacherDocumento10 páginasFred Factor TeacherVasile Busuioc100% (1)
- Curriculum Vitae SummaryDocumento5 páginasCurriculum Vitae SummaryChechoVegaAún no hay calificaciones
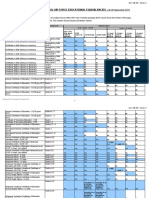
- 2022 Year 5 Dsa Selection CriteriaDocumento8 páginas2022 Year 5 Dsa Selection CriteriaMaddie BeeAún no hay calificaciones
- Kerala Higher Secondary Exam ApplicationDocumento2 páginasKerala Higher Secondary Exam ApplicationRahul Sankar60% (5)
- Department of Education: Servillano A. Arzaga, Ceso V Schools Division SuperintendentDocumento3 páginasDepartment of Education: Servillano A. Arzaga, Ceso V Schools Division SuperintendentRM FerrancolAún no hay calificaciones
- Prevention Early Identification and Intervention of DisabilitiesDocumento34 páginasPrevention Early Identification and Intervention of Disabilitiesapi-254947702100% (1)
- ARTS 1-2nd QTR WorksheetsDocumento10 páginasARTS 1-2nd QTR WorksheetsRecelyn DuranAún no hay calificaciones
- ATC Subject Activity-2021-2022-ReportDocumento9 páginasATC Subject Activity-2021-2022-ReportHarshith KAún no hay calificaciones
- ACET Topper success story - Regular study, thorough understandingDocumento1 páginaACET Topper success story - Regular study, thorough understandingSaamy KapoorAún no hay calificaciones
- Covering Letter APGLI ProposalsDocumento2 páginasCovering Letter APGLI ProposalsADONI GOVT POLYTECHNICAún no hay calificaciones
- Concept of Motivational Training To AthletesDocumento14 páginasConcept of Motivational Training To AthletesShailAún no hay calificaciones
- Nurs 2021 - Midterm EvaluationDocumento9 páginasNurs 2021 - Midterm Evaluationapi-240864098Aún no hay calificaciones
- Williams e Chesterman (2007)Documento79 páginasWilliams e Chesterman (2007)Veridiana Cunha100% (1)
- Contemporary Teacher Leadership Ass1Documento27 páginasContemporary Teacher Leadership Ass1api-357663411Aún no hay calificaciones
- Principles of Managment Star Bucks - Strategic ControlsDocumento5 páginasPrinciples of Managment Star Bucks - Strategic ControlsKevin Varner100% (1)
- Eld 307 - The Perfect Pet Lesson PlanDocumento2 páginasEld 307 - The Perfect Pet Lesson Planapi-250081618Aún no hay calificaciones
- Notification SSA HSSPP BRP PostsDocumento2 páginasNotification SSA HSSPP BRP PostsTechnical4uAún no hay calificaciones
- Construction Contract Administration TOCDocumento2 páginasConstruction Contract Administration TOCccastilloAún no hay calificaciones
- Poe - Professional InterviewDocumento7 páginasPoe - Professional Interviewapi-302341617Aún no hay calificaciones
- Istc 541 Technology in The Social Studies ClassroomDocumento11 páginasIstc 541 Technology in The Social Studies Classroomapi-606308354Aún no hay calificaciones
- Bhatt Counseling BrochureDocumento2 páginasBhatt Counseling Brochureapi-366056267Aún no hay calificaciones
- Resume For Teachers ComDocumento5 páginasResume For Teachers Comburgeafgf100% (1)
- GCU College of Education LESSON PLAN TEMPLATE: Juliette Gordon Low's Life and KindnessDocumento3 páginasGCU College of Education LESSON PLAN TEMPLATE: Juliette Gordon Low's Life and KindnessMaryum NisarAún no hay calificaciones