También podría gustarte
- Pre-Exam Preparation For Medicine (January 1, 2014) - (935152549X)Documento314 páginasPre-Exam Preparation For Medicine (January 1, 2014) - (935152549X)RinkalAún no hay calificaciones
- Just What the Doctor Ordered: The Insider’s Guide to Getting into Medical School in CanadaDe EverandJust What the Doctor Ordered: The Insider’s Guide to Getting into Medical School in CanadaAún no hay calificaciones
- House OfficerDocumento32 páginasHouse Officerapi-3705046100% (1)
- WHO Manual - The Treatment of DiarrhoeaDocumento47 páginasWHO Manual - The Treatment of DiarrhoeaRamona BunescuAún no hay calificaciones
- Pediatric Burns PowerpointDocumento29 páginasPediatric Burns Powerpointyolondanic100% (1)
- Parathyroid Gland and Other Endocrine GlandsDocumento35 páginasParathyroid Gland and Other Endocrine GlandsDrRahma Ali HeissAún no hay calificaciones
- CH 21 Obstetric AnaesthesiaDocumento39 páginasCH 21 Obstetric AnaesthesiaChristian LeepoAún no hay calificaciones
- Management of Diabetes Patients in SurgeryDocumento28 páginasManagement of Diabetes Patients in Surgerylow_sernAún no hay calificaciones
- Temp File MRCGP Revision Guide FreeBook2Documento73 páginasTemp File MRCGP Revision Guide FreeBook2Baby HanmiAún no hay calificaciones
- Green Top Guidelines 11Documento24 páginasGreen Top Guidelines 11garfield1Aún no hay calificaciones
- TESTS FOR LIVER FUNCTION Arneson BookDocumento28 páginasTESTS FOR LIVER FUNCTION Arneson Bookzahrotun nisaAún no hay calificaciones
- Examination Medicine A Guide To Physician Training PDFDocumento2 páginasExamination Medicine A Guide To Physician Training PDFJack0% (3)
- Pathophysiology of EndocrinologyDocumento25 páginasPathophysiology of EndocrinologyISRAELAún no hay calificaciones
- Update in AnaesthesiaDocumento52 páginasUpdate in AnaesthesiaRoy AAún no hay calificaciones
- Endocrinology Take Home ExamDocumento7 páginasEndocrinology Take Home ExamRenz L. SalumbreAún no hay calificaciones
- A Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsDe EverandA Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsAún no hay calificaciones
- Non Pneumatic Anti Shock Garment To Stabilize Women With Hypovolemic Shock Secondary To Obstetric HemorrhageDocumento2 páginasNon Pneumatic Anti Shock Garment To Stabilize Women With Hypovolemic Shock Secondary To Obstetric HemorrhagednnivAún no hay calificaciones
- Neonatal Circulation Changes / Unbalanced Circulation: Neonatal Cardiac Conditions: Medical and Surgical ManagementDocumento4 páginasNeonatal Circulation Changes / Unbalanced Circulation: Neonatal Cardiac Conditions: Medical and Surgical ManagementAnita Maria UlfaAún no hay calificaciones
- 04.04 Dermatologic PharmacologyDocumento3 páginas04.04 Dermatologic PharmacologyMaikka IlaganAún no hay calificaciones
- Omars GuidelinesDocumento103 páginasOmars GuidelinesAbdullahi HabibAún no hay calificaciones
- Viwa Topics - Physiology: Fluid BalanceDocumento8 páginasViwa Topics - Physiology: Fluid BalancePirabakar MahendranAún no hay calificaciones
- Telephonic RN Case ManagerDocumento2 páginasTelephonic RN Case Managerapi-78703590Aún no hay calificaciones
- The Multi-Organ Donor: A Guide to Selection, Preservation and ProcurementDe EverandThe Multi-Organ Donor: A Guide to Selection, Preservation and ProcurementCalificación: 5 de 5 estrellas5/5 (1)
- OSCE ReviewDocumento45 páginasOSCE ReviewKay BristolAún no hay calificaciones
- Paediatric Clerkship Manual 2013-2014Documento33 páginasPaediatric Clerkship Manual 2013-2014neo12w100% (2)
- Mechanical Ventilation Handout - AllenhoDocumento22 páginasMechanical Ventilation Handout - Allenhofriyaz8197100% (1)
- High Yield SurgeryDocumento77 páginasHigh Yield SurgeryDr.2020Aún no hay calificaciones
- Anti Hypertensive Drugs - ACE InhibitorDocumento16 páginasAnti Hypertensive Drugs - ACE InhibitorApurba Sarker Apu100% (1)
- History Taking: DR - Ahmed Gaber Ass. Prof of Neurology Ain Shams UniversityDocumento81 páginasHistory Taking: DR - Ahmed Gaber Ass. Prof of Neurology Ain Shams UniversityKhaled OssamaAún no hay calificaciones
- 09 - Congenital SyndromesDocumento76 páginas09 - Congenital SyndromesROHIT100% (1)
- Csa TemplateDocumento14 páginasCsa Templatemyat25Aún no hay calificaciones
- RCOG Guideline 2011Documento24 páginasRCOG Guideline 2011John DoeAún no hay calificaciones
- 2009432Documento32 páginas2009432Luis Alberto Letona QuispeAún no hay calificaciones
- Renal Artery Stenosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe EverandRenal Artery Stenosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsCalificación: 5 de 5 estrellas5/5 (1)
- Handout 11 Electrolyte DisordersDocumento14 páginasHandout 11 Electrolyte DisordersGrape Juice100% (1)
- Clinicalmedicine Notes OsceDocumento18 páginasClinicalmedicine Notes OsceSindu Sai0% (1)
- ABG InterpretationDocumento11 páginasABG InterpretationertrggerAún no hay calificaciones
- The Inflammatory ProcessDe EverandThe Inflammatory ProcessBenjamin W. ZweifachAún no hay calificaciones
- ABC of AlcoholDe EverandABC of AlcoholAnne McCuneAún no hay calificaciones
- 00 Obs&Gyn Clerkship-1-1Documento9 páginas00 Obs&Gyn Clerkship-1-1samwel daniel100% (1)
- Pharmacology of Cardiac Function: Section of Pharmacology of the International Union of Physiological SciencesDe EverandPharmacology of Cardiac Function: Section of Pharmacology of the International Union of Physiological SciencesOtto KrayerAún no hay calificaciones
- Analgesia For Labor and Vaginal DeliveryDocumento94 páginasAnalgesia For Labor and Vaginal DeliverynijasAún no hay calificaciones
- Maslach 01 JobburnoutDocumento28 páginasMaslach 01 JobburnoutJuan Perez100% (1)
- Endocrinology - Dr. R. SilverDocumento44 páginasEndocrinology - Dr. R. SilverOmoloye AyooluwaAún no hay calificaciones
- OSCE Reasoning and ConditionsDocumento111 páginasOSCE Reasoning and ConditionsWiCKieWiCKAún no hay calificaciones
- Paediatric UrologyDocumento194 páginasPaediatric UrologyTrishenth FonsekaAún no hay calificaciones
- Kidney TransplantationDocumento14 páginasKidney TransplantationSujith KuttanAún no hay calificaciones
- COMPLETE Medical Disease in PregnancyDocumento210 páginasCOMPLETE Medical Disease in PregnancyCHANDREN ARUMUGAMAún no hay calificaciones
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAún no hay calificaciones
- Antibiotics in SurgeryDocumento18 páginasAntibiotics in SurgeryGiovanni HenryAún no hay calificaciones
- Bronchure PTSDDocumento3 páginasBronchure PTSDChristian LeepoAún no hay calificaciones
- CH 46 Complications of AnaesthesiaDocumento29 páginasCH 46 Complications of AnaesthesiaChristian LeepoAún no hay calificaciones
- CH 19 Spinal AnaesthesiaDocumento29 páginasCH 19 Spinal AnaesthesiaChristian Leepo100% (1)
- CH 13 Low Cost EquipmentDocumento16 páginasCH 13 Low Cost EquipmentChristian LeepoAún no hay calificaciones
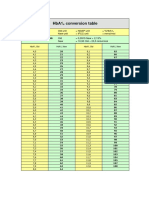
- HbA1cConversionTable PDFDocumento1 páginaHbA1cConversionTable PDFDarkoMaxAún no hay calificaciones
- Carbohydrates - Part - 2 - MazenDocumento28 páginasCarbohydrates - Part - 2 - MazenAhmed GaberAún no hay calificaciones
- D1 001 Prof Rudi STAR - DM in Indonesia - From Theory To The Real WorldDocumento37 páginasD1 001 Prof Rudi STAR - DM in Indonesia - From Theory To The Real WorldNovietha Lia FarizymelinAún no hay calificaciones
- Yuwell Accusure 510 ManualDocumento20 páginasYuwell Accusure 510 Manualrepolho1234Aún no hay calificaciones
- Ispad 2022Documento477 páginasIspad 2022hakimadnenAún no hay calificaciones
- Diabetis ThesisDocumento23 páginasDiabetis ThesisHannah CaldinoAún no hay calificaciones
- Hypoglycemia in Adults With Diabetes MellitusDocumento25 páginasHypoglycemia in Adults With Diabetes MellitusEsra AljafferAún no hay calificaciones
- ICD DiabetesDocumento4 páginasICD DiabetesfadhilahAún no hay calificaciones
- Trisula DM Titis Bang ErikDocumento56 páginasTrisula DM Titis Bang ErikTitisAún no hay calificaciones
- Diabetes MellitusDocumento8 páginasDiabetes MellitusJaja RamosAún no hay calificaciones
- Diabetes MellitusDocumento17 páginasDiabetes MellitusRuqayya KobatteAún no hay calificaciones
- St. Stephen's Hospital: Dept of Endocrinology, Diabetes & Metabolic MedicineDocumento6 páginasSt. Stephen's Hospital: Dept of Endocrinology, Diabetes & Metabolic MedicineDr ratna kumariAún no hay calificaciones
- P4 Team BDocumento8 páginasP4 Team BPranali WaghodeAún no hay calificaciones
- PMC4020327-jdi 12214Documento11 páginasPMC4020327-jdi 12214anca irinaAún no hay calificaciones
- t2dm Class Comparions ChartDocumento1 páginat2dm Class Comparions Chartpinkup1199Aún no hay calificaciones
- Insulin: Making Sense of Current OptionsDocumento30 páginasInsulin: Making Sense of Current OptionsSERGIO LOPEZAún no hay calificaciones
- Stress Hyperglycemia: Anand MosesDocumento4 páginasStress Hyperglycemia: Anand MosesDaeng Arya01Aún no hay calificaciones
- 15 Easy Ways To Lower Blood Sugar Levels NaturallyDocumento12 páginas15 Easy Ways To Lower Blood Sugar Levels NaturallyJ SmithAún no hay calificaciones
- J. Biol. Chem.-1941-Somogyi-219-27Documento10 páginasJ. Biol. Chem.-1941-Somogyi-219-27gibrambo5770Aún no hay calificaciones
- ReportsDocumento15 páginasReportsamandio silvaAún no hay calificaciones
- Risk Factors For DiabetesDocumento2 páginasRisk Factors For Diabetesmainehoona100% (1)
- Antidiabetic Drugs: Raymund N. Tapaoan, RPHDocumento23 páginasAntidiabetic Drugs: Raymund N. Tapaoan, RPHNicole EncinaresAún no hay calificaciones
- Powerpoint Presentation On DiabetesDocumento15 páginasPowerpoint Presentation On DiabetesAbbeyBandola0% (1)
- Antidiabetic Drug PDFDocumento91 páginasAntidiabetic Drug PDFAlifia ainushAún no hay calificaciones
- Diabetes PPT FianlDocumento31 páginasDiabetes PPT FianlUqba MishalAún no hay calificaciones
- هاله خالد عطا الله عرارDocumento2 páginasهاله خالد عطا الله عرارHala ArarAún no hay calificaciones
- CMScript 1 of 2017Documento3 páginasCMScript 1 of 2017Silvia RAún no hay calificaciones
- Resume Latar BelakangDocumento22 páginasResume Latar BelakangAngelika MayaAún no hay calificaciones
- Exercise 4 - RRLDocumento12 páginasExercise 4 - RRLNOREEN MITZI LOPEZAún no hay calificaciones