También podría gustarte
- Vit ADocumento4 páginasVit AchauhannareshAún no hay calificaciones
- Beet Root Juice On Haemoglobin Among Adolescent GirlsDocumento5 páginasBeet Root Juice On Haemoglobin Among Adolescent GirlsRaras PraminingrumAún no hay calificaciones
- Iron-Deficiency Anemia Among Children in Southwest IranDocumento7 páginasIron-Deficiency Anemia Among Children in Southwest IrandooocAún no hay calificaciones
- Perbedaan Kadar Seng Serum Dan Kadar C-Reactive Protein Pada Anak Balita Dengan Kadar Serum Retinol Normal Dan Tidak NormalDocumento6 páginasPerbedaan Kadar Seng Serum Dan Kadar C-Reactive Protein Pada Anak Balita Dengan Kadar Serum Retinol Normal Dan Tidak NormalLampuPijarAún no hay calificaciones
- Determinants of Nutritional Anaemia in Children Less Than Five Years AgeDocumento6 páginasDeterminants of Nutritional Anaemia in Children Less Than Five Years AgeBaiiqDelaYulianingtyasAún no hay calificaciones
- Giardiasis and Poor Vitamin A Status Among Aboriginal School Children in Rural MalaysiaDocumento5 páginasGiardiasis and Poor Vitamin A Status Among Aboriginal School Children in Rural Malaysiaevandere19Aún no hay calificaciones
- Rol EditedDocumento9 páginasRol EditedDani PhilipAún no hay calificaciones
- Suplementasi Vitamin A Dan Asupan Zat Gizi Dengan Serum Retinol Dan Morbiditas Anak 1-3 TahunDocumento9 páginasSuplementasi Vitamin A Dan Asupan Zat Gizi Dengan Serum Retinol Dan Morbiditas Anak 1-3 TahundhannylagarenseAún no hay calificaciones
- Correlation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaDocumento4 páginasCorrelation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaOmWawanAún no hay calificaciones
- Profile of Severe Nutritional Anemia in Children at A Tertiary Care Hospital, South IndiaDocumento8 páginasProfile of Severe Nutritional Anemia in Children at A Tertiary Care Hospital, South IndiaDr. Krishna N. SharmaAún no hay calificaciones
- Effects of Vitamin A, Vitamin A Plus Zinc, and Multiple Micronutrients On Anemia in Preschool Children in Chongqing, ChinaDocumento10 páginasEffects of Vitamin A, Vitamin A Plus Zinc, and Multiple Micronutrients On Anemia in Preschool Children in Chongqing, ChinaFentiAún no hay calificaciones
- Diet Quality and Nutritional Status of Rural Adolescent Girl Beneficiaries of ICDS in North IndiaDocumento10 páginasDiet Quality and Nutritional Status of Rural Adolescent Girl Beneficiaries of ICDS in North Indiameenakshi_decemberAún no hay calificaciones
- Nutri5 PDFDocumento3 páginasNutri5 PDFfkkfoxAún no hay calificaciones
- Prevalence of Anaemia Among Adolescent Girls: A Cross Sectional Exploratory StudyDocumento3 páginasPrevalence of Anaemia Among Adolescent Girls: A Cross Sectional Exploratory StudyJamilaAún no hay calificaciones
- Stunting Mesir PDFDocumento9 páginasStunting Mesir PDFRina HudayaAún no hay calificaciones
- The Difference of Urinary Neutrophil Gelatinase-Associated Lipocalin Levels in Moderate Malnutrition and Well-Nutrition in School-Age ChildrenDocumento5 páginasThe Difference of Urinary Neutrophil Gelatinase-Associated Lipocalin Levels in Moderate Malnutrition and Well-Nutrition in School-Age Childrenasri rachmawatiAún no hay calificaciones
- JurnalDocumento4 páginasJurnalLee Ji EunAún no hay calificaciones
- Nutritional Status of School Age Children (5-14 Years) in A Rural Health Block of North India (Kashmir) Using WHO Z-Score SystemDocumento3 páginasNutritional Status of School Age Children (5-14 Years) in A Rural Health Block of North India (Kashmir) Using WHO Z-Score SystemrswonolAún no hay calificaciones
- Nutritional Status and Dietary Intakes of Children Aged 6 Months To 12 Years Findings of The Nutrition Survey of Malaysian Children Seanuts MalaysiaDocumento15 páginasNutritional Status and Dietary Intakes of Children Aged 6 Months To 12 Years Findings of The Nutrition Survey of Malaysian Children Seanuts MalaysiaNadiah Umniati SyarifahAún no hay calificaciones
- Adequate Vitamin A Levels With Stunting Adolescents of Minangkabau Ethnicity in Indonesia-A Case Control StudyDocumento4 páginasAdequate Vitamin A Levels With Stunting Adolescents of Minangkabau Ethnicity in Indonesia-A Case Control Studyjesimawarni777Aún no hay calificaciones
- Prevalence and Risk Factors of Anemia in Under Five-Year-Old Children in Children's HospitalDocumento4 páginasPrevalence and Risk Factors of Anemia in Under Five-Year-Old Children in Children's Hospitalindahsarizahab 28Aún no hay calificaciones
- Ekstrak Kelopak Bunga Rosella Untuk Anemia RemajaDocumento8 páginasEkstrak Kelopak Bunga Rosella Untuk Anemia RemajaLuluk handayaniAún no hay calificaciones
- Knowledge About Iron Rich Foods and Its Consumption Pattern Among Adolescent Girls in An Urban Slum of KolarDocumento6 páginasKnowledge About Iron Rich Foods and Its Consumption Pattern Among Adolescent Girls in An Urban Slum of KolarFaseehaAún no hay calificaciones
- Isqr PDFDocumento7 páginasIsqr PDFOmy NataliaAún no hay calificaciones
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Documento6 páginasP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)galihrahman51Aún no hay calificaciones
- 8729 24611 1 SM PDFDocumento8 páginas8729 24611 1 SM PDFnevaAún no hay calificaciones
- Building A Prediction Model FoDocumento9 páginasBuilding A Prediction Model Fosyukrianti syahdaAún no hay calificaciones
- AnaemiaDocumento14 páginasAnaemiasaima hanifAún no hay calificaciones
- Status Vitamin A Anak 12 59 Bulan Dan CADocumento10 páginasStatus Vitamin A Anak 12 59 Bulan Dan CALastrie BuluatieAún no hay calificaciones
- Magnesium Deficiency and Its Lack of Association With Asthma in Taiwanese Elementary School ChildrenDocumento7 páginasMagnesium Deficiency and Its Lack of Association With Asthma in Taiwanese Elementary School ChildrenSukma EffendyAún no hay calificaciones
- Vol 05 Issue 02 Section: Healthcare Category: Research Received On: 02/12/12 Revised On: 27/12/12 Accepted On: 16/01/13Documento6 páginasVol 05 Issue 02 Section: Healthcare Category: Research Received On: 02/12/12 Revised On: 27/12/12 Accepted On: 16/01/13Dwitiara SeptianiAún no hay calificaciones
- Daily Consumption of Growing-Up Milk Is Associated With Less Stunting Among Indonesian ToddlersDocumento7 páginasDaily Consumption of Growing-Up Milk Is Associated With Less Stunting Among Indonesian ToddlersAnugerah DestiaAún no hay calificaciones
- 287 467 1 SM PDFDocumento18 páginas287 467 1 SM PDFRaida Althafunnisa SbsAún no hay calificaciones
- Cover Page To AbstractDocumento12 páginasCover Page To Abstractvikram pratap singhAún no hay calificaciones
- Anemia in Pre-School Children-Does Time Change Anything?Documento5 páginasAnemia in Pre-School Children-Does Time Change Anything?NZ FreelancersAún no hay calificaciones
- 1824-Article Text-6890-1-10-20220428Documento8 páginas1824-Article Text-6890-1-10-20220428tinodbsAún no hay calificaciones
- Revisi: Gambaran Asupan Vitamin A, Kadar Serum Seng, Dan Status Gizi Pada Anak Usia 9-12 TahunDocumento17 páginasRevisi: Gambaran Asupan Vitamin A, Kadar Serum Seng, Dan Status Gizi Pada Anak Usia 9-12 TahunPrema Piscerletapio KickAún no hay calificaciones
- Revisi: Gambaran Asupan Vitamin A, Kadar Serum Seng, Dan Status Gizi Pada Anak Usia 9-12 TahunDocumento17 páginasRevisi: Gambaran Asupan Vitamin A, Kadar Serum Seng, Dan Status Gizi Pada Anak Usia 9-12 TahunPrema Piscerletapio KickAún no hay calificaciones
- RandomizedDocumento7 páginasRandomizedmechi_ghisyaAún no hay calificaciones
- Artikel 2Documento7 páginasArtikel 2Claudia BuheliAún no hay calificaciones
- 1 Arif PDFDocumento10 páginas1 Arif PDFDevy Wulan DariAún no hay calificaciones
- Composition of Chicken Liver Nugget To Organoleptic and Hemoglobin Levels in The Efforts To Prevent Adolescent Female AnemiaDocumento5 páginasComposition of Chicken Liver Nugget To Organoleptic and Hemoglobin Levels in The Efforts To Prevent Adolescent Female AnemiaFarhiyah IsnaeniAún no hay calificaciones
- Prevalenceof Vitamin b12 Deficiency in Highersocio-Economical Class Ofbhuj-KutchDocumento3 páginasPrevalenceof Vitamin b12 Deficiency in Highersocio-Economical Class Ofbhuj-KutchIOSR Journal of PharmacyAún no hay calificaciones
- 2809 250 PBDocumento8 páginas2809 250 PBAndi RahmadAún no hay calificaciones
- Milk On and Bone MineralDocumento8 páginasMilk On and Bone MineralJeremia Kevin EmEmAún no hay calificaciones
- Prevalence of Iron-Deficiency Anaemia Among University Students in Noakhali Region, BangladeshDocumento8 páginasPrevalence of Iron-Deficiency Anaemia Among University Students in Noakhali Region, BangladeshFitrah RahmadhaniAún no hay calificaciones
- TYQA Vitamin D DeficiencyDocumento13 páginasTYQA Vitamin D DeficiencyPratiwi Dwi LestariAún no hay calificaciones
- Albumin and Serum Vitamin A Status of Malnourished ChildrenDocumento6 páginasAlbumin and Serum Vitamin A Status of Malnourished ChildrenVidinikusumaAún no hay calificaciones
- Naskah Publikasi-204Documento8 páginasNaskah Publikasi-204Achmad YunusAún no hay calificaciones
- Dietary KemmeDocumento5 páginasDietary KemmeLeighvan PapasinAún no hay calificaciones
- The Marketing Tacticsused For Selling Artificially Processed Food &its Impact On Child HealthDocumento14 páginasThe Marketing Tacticsused For Selling Artificially Processed Food &its Impact On Child HealthTJPRC PublicationsAún no hay calificaciones
- Association Between Serum Vitamin A Levels and Recurrent Respiratory Tract Infections in ChildrenDocumento9 páginasAssociation Between Serum Vitamin A Levels and Recurrent Respiratory Tract Infections in Childrenjulio cesarAún no hay calificaciones
- Prema Ramachandran: Director Nutrition Foundation of India and President, National Academy of Medical SciencesDocumento46 páginasPrema Ramachandran: Director Nutrition Foundation of India and President, National Academy of Medical SciencesSumeet VasandaniAún no hay calificaciones
- Prevention and Control of Anemia Amongst Children IndiaDocumento9 páginasPrevention and Control of Anemia Amongst Children IndiaafrinaAún no hay calificaciones
- Assessment of Vitamin B-6 Estimated Average RequirDocumento5 páginasAssessment of Vitamin B-6 Estimated Average RequirUlfa Mudia SariAún no hay calificaciones
- IJP - Volume 5 - Issue 12 - Pages 6245-6252Documento8 páginasIJP - Volume 5 - Issue 12 - Pages 6245-6252Rayhand MubarakhAún no hay calificaciones
- BJN Vol 110 S3S0007114513002110aDocumento9 páginasBJN Vol 110 S3S0007114513002110aizzul widadAún no hay calificaciones
- BHS InggrisDocumento9 páginasBHS InggrisAies AishaAún no hay calificaciones
- Complementary and Alternative Medical Lab Testing Part 7: EndocrineDe EverandComplementary and Alternative Medical Lab Testing Part 7: EndocrineAún no hay calificaciones
- Complementary and Alternative Medical Lab Testing Part 16: HematologyDe EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyAún no hay calificaciones
- Oxidant Stress in Primary Nephrotic Syndrome: Does It Modulate The Response To Corticosteroids?Documento6 páginasOxidant Stress in Primary Nephrotic Syndrome: Does It Modulate The Response To Corticosteroids?galihrahman51Aún no hay calificaciones
- Podocyte Injury: The Role of Proteinuria, Urinary Plasminogen, and Oxidative StressDocumento10 páginasPodocyte Injury: The Role of Proteinuria, Urinary Plasminogen, and Oxidative Stressgalihrahman51Aún no hay calificaciones
- Biomol SN InvivoDocumento11 páginasBiomol SN Invivogalihrahman51Aún no hay calificaciones
- Stres Oksidative SN 2021Documento11 páginasStres Oksidative SN 2021galihrahman51Aún no hay calificaciones
- Podocyte InjuryDocumento17 páginasPodocyte Injurygalihrahman51Aún no hay calificaciones
- HARGADocumento15 páginasHARGAgalihrahman51Aún no hay calificaciones
- MR 31 Jan 2021 - BronkopneumoniaDocumento30 páginasMR 31 Jan 2021 - Bronkopneumoniagalihrahman51Aún no hay calificaciones
- Ophthalmol Clin. 2011 51 (3) : 27-36: Daftar PustakaDocumento2 páginasOphthalmol Clin. 2011 51 (3) : 27-36: Daftar Pustakagalihrahman51Aún no hay calificaciones
- Emergency Case Report December, 18 - , 19 2013: Resident On Duty: Dr. Alex Chief On Duty: Galih RahmanDocumento66 páginasEmergency Case Report December, 18 - , 19 2013: Resident On Duty: Dr. Alex Chief On Duty: Galih Rahmangalihrahman51Aún no hay calificaciones
- Serum Total Proteins and Vitamin A Levels of Adolescent Girls (10-15 Years) Attending A Government School in Jaipur City, IndiaDocumento4 páginasSerum Total Proteins and Vitamin A Levels of Adolescent Girls (10-15 Years) Attending A Government School in Jaipur City, Indiagalihrahman51Aún no hay calificaciones
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Documento6 páginasP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)galihrahman51Aún no hay calificaciones
- Konjungtivitis Alergika: Laporan KasusDocumento3 páginasKonjungtivitis Alergika: Laporan Kasusgalihrahman51Aún no hay calificaciones
- 6 Essential NutrientsDocumento5 páginas6 Essential NutrientsJairo GarciaAún no hay calificaciones
- Fertilizer IndustryDocumento27 páginasFertilizer Industryshamanth143kAún no hay calificaciones
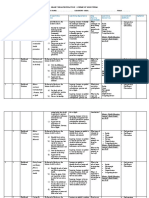
- Grade 7 SchemesDocumento7 páginasGrade 7 SchemesMalesi SiemaAún no hay calificaciones
- Technical Info Librel Fe-DPDocumento4 páginasTechnical Info Librel Fe-DPRijalul AuthonAún no hay calificaciones
- Fortified TeaDocumento12 páginasFortified TeaRahul TripathiAún no hay calificaciones
- RA 8172 - Asin Law - 2Documento22 páginasRA 8172 - Asin Law - 2Maxine Alexandra JaimeAún no hay calificaciones
- CRP FISH Proposal PDFDocumento287 páginasCRP FISH Proposal PDFNujhat SharminAún no hay calificaciones
- Pramotion Nutrint ImpDocumento46 páginasPramotion Nutrint ImpRahul SableAún no hay calificaciones
- NESTLE Kasambuhay Program - GRP1Documento30 páginasNESTLE Kasambuhay Program - GRP1Zheanne ClaireAún no hay calificaciones
- Assignment ON IPM-FFSDocumento4 páginasAssignment ON IPM-FFSCherry Mae Claire Villanueva-GomezAún no hay calificaciones
- Zinc (ZN) Importance For Crop Production - A ReviewDocumento5 páginasZinc (ZN) Importance For Crop Production - A ReviewLeonides Bernardo Fernández LicónAún no hay calificaciones
- Nebiyu Proposal HIV AND NUTRTIONDocumento28 páginasNebiyu Proposal HIV AND NUTRTIONBinkisa BilloAún no hay calificaciones
- Your Brain On FoodDocumento2 páginasYour Brain On FoodRusso Dalmasso50% (2)
- A. Qureshi, Et AlDocumento11 páginasA. Qureshi, Et AlAr Kuldeep MalamAún no hay calificaciones
- Health Care Programs - DOHDocumento46 páginasHealth Care Programs - DOHZarlyn MirafloresAún no hay calificaciones
- National Nutrition ProgramDocumento20 páginasNational Nutrition Programsabaiq2003Aún no hay calificaciones
- Hul Launches Brooke Bond Sehatmand A Tea With Vitamins - tcm1255 463861 - en PDFDocumento2 páginasHul Launches Brooke Bond Sehatmand A Tea With Vitamins - tcm1255 463861 - en PDFRiturajPaulAún no hay calificaciones
- Cobb500 Broiler Performance Nutrition Supplement (English)Documento14 páginasCobb500 Broiler Performance Nutrition Supplement (English)Eko SantosoAún no hay calificaciones
- Project On SaltDocumento8 páginasProject On Saltbulbul12Aún no hay calificaciones
- Skinny Fat Solution The 2 Phases of A SFTDocumento50 páginasSkinny Fat Solution The 2 Phases of A SFTcharlie100% (2)
- Food & Nutrition Security - Position PaperDocumento18 páginasFood & Nutrition Security - Position PaperdennysonAún no hay calificaciones
- Tos 2nd Periodical Test Mapeh 7Documento6 páginasTos 2nd Periodical Test Mapeh 7Maribel CelisAún no hay calificaciones
- Production, Chemical and Sensory Evaluation of Cookies Fortified With Moringa Oleifera LeavesDocumento8 páginasProduction, Chemical and Sensory Evaluation of Cookies Fortified With Moringa Oleifera Leavesayele asefaAún no hay calificaciones
- Neglected and Underutilized Crop Species The Key To Improving Soil Nutritional Security For Fighting Poverty, Hunger and Malnutrition in North-Western IGP: A ReviewDocumento8 páginasNeglected and Underutilized Crop Species The Key To Improving Soil Nutritional Security For Fighting Poverty, Hunger and Malnutrition in North-Western IGP: A Reviewatul211988Aún no hay calificaciones
- Nutrition Training ManualDocumento86 páginasNutrition Training ManualdennysonAún no hay calificaciones
- Anshul Products BookletDocumento28 páginasAnshul Products BookletSunil ShamanurAún no hay calificaciones
- Sports Nutrition - Vitamins and Trace Elements (2nd Ed.) Volume of Nutrition in Exercise and Sport Series - CRC-Taylor & Francis (PDFDrive - Com) - Copia - Parte1Documento20 páginasSports Nutrition - Vitamins and Trace Elements (2nd Ed.) Volume of Nutrition in Exercise and Sport Series - CRC-Taylor & Francis (PDFDrive - Com) - Copia - Parte1RJAún no hay calificaciones
- Micronutrient Supplementation: Alma Magdasoc-Lozada, RND, Mapa, PHD Pa Nutritionist - Dietitian IV DOH RO V, Legazpi CityDocumento46 páginasMicronutrient Supplementation: Alma Magdasoc-Lozada, RND, Mapa, PHD Pa Nutritionist - Dietitian IV DOH RO V, Legazpi CityClaribel Domingo BayaniAún no hay calificaciones
- Doh Health Programs (Child Program)Documento64 páginasDoh Health Programs (Child Program)Wilma Nierva BeraldeAún no hay calificaciones
- Anaemia Policy BriefDocumento7 páginasAnaemia Policy BriefAini DjunetAún no hay calificaciones