También podría gustarte
- 10.1007/978 3 319 45333 0Documento397 páginas10.1007/978 3 319 45333 0محمد عبداللهAún no hay calificaciones
- Clinician's Manual On Autism Spectrum DisorderDocumento101 páginasClinician's Manual On Autism Spectrum Disorderمحمد عبدالله100% (1)
- Web 2.0 Applications Assignment 2013Documento7 páginasWeb 2.0 Applications Assignment 2013محمد عبدالله100% (1)
- Collaborative LearningDocumento11 páginasCollaborative LearningEFL Classroom 2.0100% (1)
- Giilbahar Tinmaz Implementing PJBL PDFDocumento19 páginasGiilbahar Tinmaz Implementing PJBL PDFWisnubangkitAún no hay calificaciones
- 1369 10502 2 SPDocumento5 páginas1369 10502 2 SPمحمد عبداللهAún no hay calificaciones
- Digital Citizen - Wikipedia, The Free EncyclopediaDocumento4 páginasDigital Citizen - Wikipedia, The Free Encyclopediaمحمد عبداللهAún no hay calificaciones
- The A1C Test and DiabetesDocumento12 páginasThe A1C Test and Diabetesمحمد عبداللهAún no hay calificaciones
- Building An E-Portfolio Learning Model: Goal Orientation and Metacognitive StrategiesDocumento21 páginasBuilding An E-Portfolio Learning Model: Goal Orientation and Metacognitive Strategiesمحمد عبداللهAún no hay calificaciones
- Learning2.0: The Impact of Web2.0 Innovation On Education and TrainingDocumento38 páginasLearning2.0: The Impact of Web2.0 Innovation On Education and Trainingapi-26175382Aún no hay calificaciones
- Web 20 1231448426732710 2Documento13 páginasWeb 20 1231448426732710 2محمد عبداللهAún no hay calificaciones
- Herbs That Lower Blood Sugar: Click Here To Email This ArticleDocumento5 páginasHerbs That Lower Blood Sugar: Click Here To Email This ArticleEdy Tagz TaguiamAún no hay calificaciones
- Anion GapDocumento2 páginasAnion Gapمحمد عبداللهAún no hay calificaciones
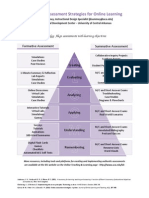
- Assessment StrategiesDocumento1 páginaAssessment Strategiesمحمد عبداللهAún no hay calificaciones
- Acid Base TutDocumento10 páginasAcid Base Tutمحمد عبداللهAún no hay calificaciones
- 6093Documento8 páginas6093محمد عبداللهAún no hay calificaciones
- 2007 NMC Summer Conference ProceedingsDocumento132 páginas2007 NMC Summer Conference Proceedingsمحمد عبداللهAún no hay calificaciones
- Web 2.0 Applications Assignment 2013Documento7 páginasWeb 2.0 Applications Assignment 2013محمد عبدالله100% (1)
- PhdmoDocumento6 páginasPhdmoمحمد عبداللهAún no hay calificaciones
- Learning2.0: The Impact of Web2.0 Innovation On Education and TrainingDocumento38 páginasLearning2.0: The Impact of Web2.0 Innovation On Education and Trainingapi-26175382Aún no hay calificaciones
- Learning2.0: The Impact of Web2.0 Innovation On Education and TrainingDocumento38 páginasLearning2.0: The Impact of Web2.0 Innovation On Education and Trainingapi-26175382Aún no hay calificaciones
- Facebook in Education: Students, Teachers, and Library PerspectivesDocumento9 páginasFacebook in Education: Students, Teachers, and Library PerspectivesJournal of ComputingAún no hay calificaciones
- AAEEBL CFP - 2013 Annual ConferenceDocumento8 páginasAAEEBL CFP - 2013 Annual Conferenceمحمد عبداللهAún no hay calificaciones
- ZULAN v2 n2Documento4 páginasZULAN v2 n2محمد عبداللهAún no hay calificaciones
- Amazing Web 2 Projects 2 Online VersionDocumento121 páginasAmazing Web 2 Projects 2 Online VersionTerry FreedmanAún no hay calificaciones
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Multiple Choice Questions-Acid Base BalanceDocumento6 páginasMultiple Choice Questions-Acid Base BalanceIdrissa Conteh100% (1)
- Approach To Acid-Base Disorders: Quran 5:32Documento34 páginasApproach To Acid-Base Disorders: Quran 5:32Hina BatoolAún no hay calificaciones
- Intern Survival Guide: DisclaimerDocumento23 páginasIntern Survival Guide: DisclaimerKing David100% (1)
- Arterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPDocumento39 páginasArterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPGio Tamaño BalisiAún no hay calificaciones
- Acid Base BalanceDocumento40 páginasAcid Base Balancemohdmaghyreh100% (1)
- Acid-Base Disorders in The Critically Ill PatientDocumento11 páginasAcid-Base Disorders in The Critically Ill PatientAniAliciaOrtizCastleAún no hay calificaciones
- Acid Base WorkshopDocumento71 páginasAcid Base WorkshopLSU Nephrology Transplant Dialysis AccessAún no hay calificaciones
- American Thoracic Society - Interpretation of Arterial Blood Gases (ABGs)Documento7 páginasAmerican Thoracic Society - Interpretation of Arterial Blood Gases (ABGs)humberto_2Aún no hay calificaciones
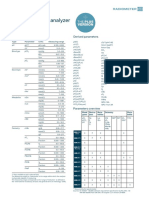
- MAPSSS000188 R2 ABL800 FLEX PLUS Specs - EN - LowDocumento2 páginasMAPSSS000188 R2 ABL800 FLEX PLUS Specs - EN - LowmemddrAún no hay calificaciones
- Toxicology Update A Rational Approach To Managing The Poisoned PatientDocumento28 páginasToxicology Update A Rational Approach To Managing The Poisoned PatientMaria Isaura Méndez OrtegaAún no hay calificaciones
- Acid Base DisordersDocumento66 páginasAcid Base DisordersIvan HensonAún no hay calificaciones
- Kalkulator AGDDocumento2 páginasKalkulator AGDMuliaAún no hay calificaciones
- Anaesthesia For TURPDocumento6 páginasAnaesthesia For TURPMutia FarinaAún no hay calificaciones
- Acid Base BalanceDocumento44 páginasAcid Base BalanceKenny JapAún no hay calificaciones
- 01 Moles WaterDocumento22 páginas01 Moles WaterJoel Topf100% (3)
- Synthesis 3 Jay VillasotoDocumento6 páginasSynthesis 3 Jay VillasotoJay VillasotoAún no hay calificaciones
- Acid-Base BalanceDocumento47 páginasAcid-Base BalanceEmmanuel RocksonAún no hay calificaciones
- Protocol - ABG Analysis by DR FazalDocumento2 páginasProtocol - ABG Analysis by DR FazalSalmanAún no hay calificaciones
- Acid Base ImbalanceDocumento50 páginasAcid Base ImbalanceDian Pratiwi BurnamaAún no hay calificaciones
- i-STAT Alinity V: Utilization GuideDocumento8 páginasi-STAT Alinity V: Utilization GuideTony ChenAún no hay calificaciones
- Understanding Acid-Base ImbalancesDocumento47 páginasUnderstanding Acid-Base ImbalancesMilikPremiumstock90Aún no hay calificaciones
- ABG Made EasyDocumento42 páginasABG Made EasyMahima LakhanpalAún no hay calificaciones
- Acid Base Disorders: It Ain'T All That Simple DR Alex Hieatt Consultant EdDocumento26 páginasAcid Base Disorders: It Ain'T All That Simple DR Alex Hieatt Consultant Edamrutha vsAún no hay calificaciones
- CANINE-Hematologic and Serum Biochemical Reference Values in Retired GreyhoundsDocumento6 páginasCANINE-Hematologic and Serum Biochemical Reference Values in Retired Greyhoundstaner_soysurenAún no hay calificaciones
- Joslin Guidelines - Uncontrolled Glucose in The Hospitalized Adult 09-26-2007Documento6 páginasJoslin Guidelines - Uncontrolled Glucose in The Hospitalized Adult 09-26-2007joslindocu100% (1)
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults: TreatmentDocumento35 páginasDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults: TreatmentyorghiLAún no hay calificaciones
- Interpretacion de AgaDocumento8 páginasInterpretacion de AgaCristhian Agustin ParedesAún no hay calificaciones
- Loresca, Kaycee-Clinical ChemistryDocumento19 páginasLoresca, Kaycee-Clinical ChemistryKaycee Gretz LorescaAún no hay calificaciones
- Diagnosis and Management of Hyperglycemic Emergencies: Hormones (Athens, Greece) October 2011Documento12 páginasDiagnosis and Management of Hyperglycemic Emergencies: Hormones (Athens, Greece) October 2011nia rahayu wAún no hay calificaciones
- Phctlec - Topic 3&4 - PrelimsDocumento24 páginasPhctlec - Topic 3&4 - PrelimsasdfdjfeonaAún no hay calificaciones