También podría gustarte
- Knowledge of Hiv Transmission and Sexual Behavior Among Zimbabwean Adolescent Females in Atlanta, Georgia: The Role of Culture and Dual SocializationDe EverandKnowledge of Hiv Transmission and Sexual Behavior Among Zimbabwean Adolescent Females in Atlanta, Georgia: The Role of Culture and Dual SocializationAún no hay calificaciones
- Overview of HIV Interventions For Young PeopleDocumento8 páginasOverview of HIV Interventions For Young PeopleCrowdOutAIDSAún no hay calificaciones
- Hiv/Aids Among Industrial & Transport WorkersDe EverandHiv/Aids Among Industrial & Transport WorkersAún no hay calificaciones
- JC2112 Synthesis Report enDocumento112 páginasJC2112 Synthesis Report enPennapa KaweewongprassertAún no hay calificaciones
- HIV MDG Factsheet WebversionDocumento2 páginasHIV MDG Factsheet WebversionFarhan KabirAún no hay calificaciones
- Young People and Hiv: HighlightsDocumento5 páginasYoung People and Hiv: HighlightsSerena SandraAún no hay calificaciones
- Tropical Med Int Health - 2019 - Finlay - Sexual and Reproductive Health Knowledge Among Adolescents in Eight Sites AcrossDocumento10 páginasTropical Med Int Health - 2019 - Finlay - Sexual and Reproductive Health Knowledge Among Adolescents in Eight Sites AcrossAhmed AbbasAún no hay calificaciones
- The United Nations and The Fight Against HIV/AIDSDocumento10 páginasThe United Nations and The Fight Against HIV/AIDSBudoy WashupapiAún no hay calificaciones
- Epidemiology of HIV and AIDS Among Adolescents 169Documento10 páginasEpidemiology of HIV and AIDS Among Adolescents 169Genevieve Caecilia Linda KAún no hay calificaciones
- PPTDocumento7 páginasPPTEviza K. NadyaAún no hay calificaciones
- Tutorial Letter 102/3/2013: Health EducationDocumento39 páginasTutorial Letter 102/3/2013: Health EducationBeNobody2Aún no hay calificaciones
- GROUP 3 Presentation On Adolescent SRH - FinalDocumento14 páginasGROUP 3 Presentation On Adolescent SRH - FinalChintu ZoboloAún no hay calificaciones
- Gender EqualityDocumento4 páginasGender EqualityTaimoor Hassan NambardaarAún no hay calificaciones
- Adolescent PregnancyDocumento60 páginasAdolescent PregnancyRafael CarrielAún no hay calificaciones
- STUDENT KAP ON HIV/AIDSDocumento22 páginasSTUDENT KAP ON HIV/AIDSbegosewAún no hay calificaciones
- 2013 Article 326Documento8 páginas2013 Article 326Ariyati MandiriAún no hay calificaciones
- 4058 99135 MakurdiDocumento111 páginas4058 99135 MakurdiSunkanmi FadojuAún no hay calificaciones
- Zimbabwe Ministry of Primary and Secondary Education Life Skills & Sexuality Education Strategy 2012-2015Documento64 páginasZimbabwe Ministry of Primary and Secondary Education Life Skills & Sexuality Education Strategy 2012-2015Yemurai Nyoni100% (2)
- HIV Interventions For Young People in The WorkplaceDocumento8 páginasHIV Interventions For Young People in The WorkplaceCrowdOutAIDSAún no hay calificaciones
- International Technical Guidance On SexuDocumento66 páginasInternational Technical Guidance On SexuClaudia GonzalesAún no hay calificaciones
- Among Youth: Hiv/AidsDocumento5 páginasAmong Youth: Hiv/AidsShahnaz RizkaAún no hay calificaciones
- Planning HivDocumento331 páginasPlanning HivCridoc DocumentationAún no hay calificaciones
- Preventing HIV/AIDS Among Young People: at The Hub of The EpidemicDocumento3 páginasPreventing HIV/AIDS Among Young People: at The Hub of The EpidemicHerdy AdrianoAún no hay calificaciones
- International Technical Guidance On Sexuality EducationDocumento66 páginasInternational Technical Guidance On Sexuality EducationAgustín DomenicaleAún no hay calificaciones
- Position Paper KENYADocumento2 páginasPosition Paper KENYAdscarmeliaAún no hay calificaciones
- Source: UNAIDS Global Summary 2006 Source: Stop Aids Now Source: Website Stop Aids Now: - UnaidsDocumento8 páginasSource: UNAIDS Global Summary 2006 Source: Stop Aids Now Source: Website Stop Aids Now: - UnaidsChindy Sagita PAún no hay calificaciones
- Zimbabwe University Paper Discusses Preventing HIV/AIDS in YouthDocumento6 páginasZimbabwe University Paper Discusses Preventing HIV/AIDS in YouthEugene MkhothamoAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Learning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSDocumento32 páginasLearning To Survive: How Education For All Would Save Millions of Young People From HIV/AIDSOxfamAún no hay calificaciones
- Support:: The Spreading of The Reproductive Health EducationDocumento34 páginasSupport:: The Spreading of The Reproductive Health EducationSavannah KhrisAún no hay calificaciones
- Final PaperDocumento13 páginasFinal Paperapi-682032779Aún no hay calificaciones
- Addressing Gender Relations in HIV Prevention Through LiteracyDocumento12 páginasAddressing Gender Relations in HIV Prevention Through LiteracyfadligmailAún no hay calificaciones
- Hif Research Paper - LMDocumento8 páginasHif Research Paper - LMapi-643319431Aún no hay calificaciones
- HIV and Conflict reportDocumento39 páginasHIV and Conflict reportTobi CrackAún no hay calificaciones
- Chapter 2: Literature ReviewDocumento26 páginasChapter 2: Literature ReviewMahal KitaAún no hay calificaciones
- eDocumento123 páginaseVishnu PrajapatAún no hay calificaciones
- International Technical Guidance On Sexuality EducationDocumento123 páginasInternational Technical Guidance On Sexuality EducationAndrei GrigoreAún no hay calificaciones
- Epidemiology of HIV and AIDS Among Adolescents 169 PDFDocumento10 páginasEpidemiology of HIV and AIDS Among Adolescents 169 PDFPAUL AYAMAHAún no hay calificaciones
- Abuja DeclarationDocumento8 páginasAbuja DeclarationChikezie OnwukweAún no hay calificaciones
- tmp129F TMPDocumento9 páginastmp129F TMPFrontiersAún no hay calificaciones
- tmp65DD TMPDocumento9 páginastmp65DD TMPFrontiersAún no hay calificaciones
- Policy On HIVAIDS EthiopiaDocumento11 páginasPolicy On HIVAIDS EthiopiaSabir Imam100% (1)
- Zamfara State School of Nursing and Midwifery, Gusau Department of Nursing Education Reproductive Health Iv Unit V: Hiv/Aids in ChildrenDocumento3 páginasZamfara State School of Nursing and Midwifery, Gusau Department of Nursing Education Reproductive Health Iv Unit V: Hiv/Aids in ChildrenNusaibat jiboAún no hay calificaciones
- ICASA 2023 Themes Advance Women, ChildrenDocumento7 páginasICASA 2023 Themes Advance Women, ChildrenmathiasAún no hay calificaciones
- India: National Youth Shadow ReportDocumento24 páginasIndia: National Youth Shadow ReportBala KumaranAún no hay calificaciones
- The State of Health in Zimbabwe Report in SummaryDocumento12 páginasThe State of Health in Zimbabwe Report in SummaryYemurai NyoniAún no hay calificaciones
- The State of Health in Zimbabwe Report in SummaryDocumento12 páginasThe State of Health in Zimbabwe Report in SummaryYemurai NyoniAún no hay calificaciones
- Hon. Nkatazo Statement On 'Criminalisation of Child Marriage' MotionDocumento3 páginasHon. Nkatazo Statement On 'Criminalisation of Child Marriage' MotionYemurai NyoniAún no hay calificaciones
- Hon. Mandipaka Statement On 'Criminalisation of Child Marriage' MotionDocumento3 páginasHon. Mandipaka Statement On 'Criminalisation of Child Marriage' MotionYemurai NyoniAún no hay calificaciones
- Hon. Matangira Statement On 'Criminalisation of Child Marriage' MotionDocumento3 páginasHon. Matangira Statement On 'Criminalisation of Child Marriage' MotionYemurai NyoniAún no hay calificaciones
- Hon. R. Moyo Statement On 'Criminalisation of Child Marriage' MotionDocumento1 páginaHon. R. Moyo Statement On 'Criminalisation of Child Marriage' MotionYemurai NyoniAún no hay calificaciones
- Hon. Mapiki Statement On 'Criminalisation of Child Marriage' MotionDocumento2 páginasHon. Mapiki Statement On 'Criminalisation of Child Marriage' MotionYemurai NyoniAún no hay calificaciones
- Child Marriage Motion SummaryDocumento29 páginasChild Marriage Motion SummaryYemurai NyoniAún no hay calificaciones
- Hon. Bunjira Statement On 'Criminalisation of Child Marriage' Motion.Documento3 páginasHon. Bunjira Statement On 'Criminalisation of Child Marriage' Motion.Yemurai NyoniAún no hay calificaciones
- Hon. Matibenga Statement On 'Criminalisation of Child Marriage' MotionDocumento3 páginasHon. Matibenga Statement On 'Criminalisation of Child Marriage' MotionYemurai NyoniAún no hay calificaciones
- Hon. Chirisa - Statement On 'Criminalisation of Child Marriage'Documento3 páginasHon. Chirisa - Statement On 'Criminalisation of Child Marriage'Yemurai NyoniAún no hay calificaciones
- Hon. Zemura Statement On 'Criminalisation of Child Marriage' MotionDocumento3 páginasHon. Zemura Statement On 'Criminalisation of Child Marriage' MotionYemurai NyoniAún no hay calificaciones
- Statement by Hon. J.F. Majome On 'Criminalisation of Child Marriage'Documento10 páginasStatement by Hon. J.F. Majome On 'Criminalisation of Child Marriage'Yemurai NyoniAún no hay calificaciones
- MOTION - 'Criminalisation of Child Marriage' Moved by Hon. Webster MaonderaDocumento6 páginasMOTION - 'Criminalisation of Child Marriage' Moved by Hon. Webster MaonderaYemurai NyoniAún no hay calificaciones
- Email Conversation With Former Zim Minister of Education D. ColtartDocumento4 páginasEmail Conversation With Former Zim Minister of Education D. ColtartYemurai NyoniAún no hay calificaciones
- Zimbabwean Chiefs' Communique On Child MarriagesDocumento3 páginasZimbabwean Chiefs' Communique On Child MarriagesYemurai NyoniAún no hay calificaciones
- End Child Marriage MotionDocumento13 páginasEnd Child Marriage MotionYemurai NyoniAún no hay calificaciones
- Petition For Legislative Changes To End Child Marriage in ZimbabweDocumento6 páginasPetition For Legislative Changes To End Child Marriage in ZimbabweYemurai NyoniAún no hay calificaciones
- Zimbabwe Ministry of Primary and Secondary Education Life Skills & Sexuality Education Strategy 2012-2015Documento64 páginasZimbabwe Ministry of Primary and Secondary Education Life Skills & Sexuality Education Strategy 2012-2015Yemurai Nyoni100% (2)
- 2014 Report On Harmful Cultural Practices Affecting Children in ZimbabweDocumento56 páginas2014 Report On Harmful Cultural Practices Affecting Children in ZimbabweYemurai Nyoni50% (2)
- Giving: By: Yemurai NyoniDocumento14 páginasGiving: By: Yemurai NyoniYemurai NyoniAún no hay calificaciones
- Aldermens SocietyDocumento6 páginasAldermens SocietyYemurai NyoniAún no hay calificaciones
- 2012 - The Release of Resurrection PowerDocumento31 páginas2012 - The Release of Resurrection PowerYemurai NyoniAún no hay calificaciones
- Clerking Edited by Nada.H.BDocumento4 páginasClerking Edited by Nada.H.BAbdulrahman NajiAún no hay calificaciones
- HIV and Islam Is HIV Prevalence Lower Am PDFDocumento6 páginasHIV and Islam Is HIV Prevalence Lower Am PDFPriyo DjatmikoAún no hay calificaciones
- Manejo RCIU Basado en EstadíosDocumento5 páginasManejo RCIU Basado en EstadíosRodrigoEscobedoAún no hay calificaciones
- ICD 9-10 - Common Codes For OBGYN-MI3859-042715Documento4 páginasICD 9-10 - Common Codes For OBGYN-MI3859-042715Avicena M IqbalAún no hay calificaciones
- Factors That Can Influence The Counselling Session - Counselling For Maternal and Newborn Health Care - Ncbi BookshelfDocumento15 páginasFactors That Can Influence The Counselling Session - Counselling For Maternal and Newborn Health Care - Ncbi BookshelfNur Ain KhadirAún no hay calificaciones
- Knowledge, Attitude and Practise Regarding Emergency Contraceptive PillsDocumento6 páginasKnowledge, Attitude and Practise Regarding Emergency Contraceptive PillsEditor IJTSRDAún no hay calificaciones
- Best Dr. Seng Shay WayDocumento8 páginasBest Dr. Seng Shay Wayhar shishAún no hay calificaciones
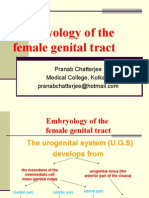
- Embryology of The Female Genital Tract: Pranab Chatterjee Medical College, KolkataDocumento31 páginasEmbryology of The Female Genital Tract: Pranab Chatterjee Medical College, KolkataPranab Chatterjee100% (4)
- Sexual Behavior of Men Who Have Sex With MenDocumento32 páginasSexual Behavior of Men Who Have Sex With MenThomas OfemAún no hay calificaciones
- Aesthetic Gynecology PDFDocumento16 páginasAesthetic Gynecology PDFBudi Iman SantosoAún no hay calificaciones
- Soal SoalDocumento3 páginasSoal SoalfirmianisaAún no hay calificaciones
- Opinion Piece Navigating Indonesia's Abortion Debate With EmpathyDocumento2 páginasOpinion Piece Navigating Indonesia's Abortion Debate With EmpathyNiko SerafinoAún no hay calificaciones
- DystociaDocumento17 páginasDystociaKarinaAún no hay calificaciones
- Assisted Reproduction Technology (ART)Documento15 páginasAssisted Reproduction Technology (ART)RPh Krishna Chandra Jagrit100% (1)
- Physiology of LaborDocumento17 páginasPhysiology of Laborsennaavia12Aún no hay calificaciones
- Ovarian New GrowthDocumento7 páginasOvarian New GrowthRegiena Tamargo100% (1)
- Tugas 1Documento20 páginasTugas 1lastia meilinaAún no hay calificaciones
- Intrauterine Device - WikipediaDocumento80 páginasIntrauterine Device - WikipediaDarshan MvAún no hay calificaciones
- Program Implementation Review - Block 5Documento20 páginasProgram Implementation Review - Block 5jollyhotdog89Aún no hay calificaciones
- 38160Documento13 páginas38160Jessa Esperanza SorioAún no hay calificaciones
- 2011-09 - Ob-GynDocumento24 páginas2011-09 - Ob-Gynsahilius100% (1)
- E TacticsDocumento22 páginasE Tacticsmaximus leodonus100% (2)
- EMMA ALICE Clinical SheetDocumento2 páginasEMMA ALICE Clinical SheetRafaela NascimentoAún no hay calificaciones
- How to do an abortion in 10 stepsDocumento5 páginasHow to do an abortion in 10 stepsShien Brojas OropesaAún no hay calificaciones
- Dagupan City Grade 12 2nd Quarter Exam ReviewDocumento4 páginasDagupan City Grade 12 2nd Quarter Exam ReviewJustin Shene ManuelAún no hay calificaciones
- Chapter One - TwoDocumento16 páginasChapter One - TwoBua NyohAún no hay calificaciones
- Step 3 - Inform All Pregnant Women of The Benefits and Management of Breastfeeding. CULTURE VariesDocumento14 páginasStep 3 - Inform All Pregnant Women of The Benefits and Management of Breastfeeding. CULTURE VariesJudith DurensAún no hay calificaciones
- MATERNALDocumento32 páginasMATERNALsean blaze100% (1)
- Antenatal Education and Postnatal Support Strategies PDFDocumento7 páginasAntenatal Education and Postnatal Support Strategies PDFNoraAún no hay calificaciones
- Amniocentesis HindiDocumento4 páginasAmniocentesis HindiRohit KumarAún no hay calificaciones
- Unwanted Advances: Sexual Paranoia Comes to CampusDe EverandUnwanted Advances: Sexual Paranoia Comes to CampusCalificación: 4 de 5 estrellas4/5 (22)
- You Can Thrive After Narcissistic Abuse: The #1 System for Recovering from Toxic RelationshipsDe EverandYou Can Thrive After Narcissistic Abuse: The #1 System for Recovering from Toxic RelationshipsCalificación: 5 de 5 estrellas5/5 (16)
- Nobody's Girl: A Memoir of Lost Innocence, Modern Day Slavery & TransformationDe EverandNobody's Girl: A Memoir of Lost Innocence, Modern Day Slavery & TransformationCalificación: 4.5 de 5 estrellas4.5/5 (33)
- Unspeakable: Surviving My Childhood and Finding My VoiceDe EverandUnspeakable: Surviving My Childhood and Finding My VoiceCalificación: 5 de 5 estrellas5/5 (59)
- The Longest Race: Inside the Secret World of Abuse, Doping, and Deception on Nike's Elite Running TeamDe EverandThe Longest Race: Inside the Secret World of Abuse, Doping, and Deception on Nike's Elite Running TeamCalificación: 5 de 5 estrellas5/5 (58)
- What Is a Girl Worth?: My Story of Breaking the Silence and Exposing the Truth about Larry Nassar and USA GymnasticsDe EverandWhat Is a Girl Worth?: My Story of Breaking the Silence and Exposing the Truth about Larry Nassar and USA GymnasticsCalificación: 4.5 de 5 estrellas4.5/5 (40)
- Letter to a Bigot: Dead But Not ForgottenDe EverandLetter to a Bigot: Dead But Not ForgottenCalificación: 4 de 5 estrellas4/5 (137)
- Tears of the Silenced: An Amish True Crime Memoir of Childhood Sexual Abuse, Brutal Betrayal, and Ultimate SurvivalDe EverandTears of the Silenced: An Amish True Crime Memoir of Childhood Sexual Abuse, Brutal Betrayal, and Ultimate SurvivalCalificación: 4.5 de 5 estrellas4.5/5 (136)
- Invisible Abuse - Instantly Spot the Covert Deception and Manipulation Tactics of Narcissists, Effortlessly Defend From and Disarm Them, and Effectively Recover: Deep Relationship Healing and RecoveryDe EverandInvisible Abuse - Instantly Spot the Covert Deception and Manipulation Tactics of Narcissists, Effortlessly Defend From and Disarm Them, and Effectively Recover: Deep Relationship Healing and RecoveryCalificación: 5 de 5 estrellas5/5 (2)
- On the Threshold of Hope: Opening the Door to Healing for Survivors of Sexual AbuseDe EverandOn the Threshold of Hope: Opening the Door to Healing for Survivors of Sexual AbuseCalificación: 5 de 5 estrellas5/5 (5)
- Fallen Idols: A Century of Screen Sex ScandalsDe EverandFallen Idols: A Century of Screen Sex ScandalsCalificación: 4 de 5 estrellas4/5 (7)
- I Love You Baby Girl... A heartbreaking true story of child abuse and neglect.De EverandI Love You Baby Girl... A heartbreaking true story of child abuse and neglect.Calificación: 3.5 de 5 estrellas3.5/5 (7)
- On Guard: Preventing and Responding to Child Abuse at ChurchDe EverandOn Guard: Preventing and Responding to Child Abuse at ChurchCalificación: 4.5 de 5 estrellas4.5/5 (6)
- Favorite Wife: Escape From PolygamyDe EverandFavorite Wife: Escape From PolygamyCalificación: 4 de 5 estrellas4/5 (73)
- Dear Professor: A Woman's Letter to Her StalkerDe EverandDear Professor: A Woman's Letter to Her StalkerCalificación: 4 de 5 estrellas4/5 (157)
- Unbound: My Story of Liberation and the Birth of the Me Too MovementDe EverandUnbound: My Story of Liberation and the Birth of the Me Too MovementCalificación: 5 de 5 estrellas5/5 (147)
- QAnon & the #Pizzagates of Hell: Unreal Tales of Occult Child Abuse by the CIADe EverandQAnon & the #Pizzagates of Hell: Unreal Tales of Occult Child Abuse by the CIACalificación: 5 de 5 estrellas5/5 (1)
- Men Who Hate Women: From Incels to Pickup Artists: The Truth about Extreme Misogyny and How it Affects Us AllDe EverandMen Who Hate Women: From Incels to Pickup Artists: The Truth about Extreme Misogyny and How it Affects Us AllCalificación: 4 de 5 estrellas4/5 (33)
- Becoming a Church that Cares Well for the AbusedDe EverandBecoming a Church that Cares Well for the AbusedCalificación: 5 de 5 estrellas5/5 (3)
- Freedom from Shame: Trauma, Forgiveness, and Healing from Sexual AbuseDe EverandFreedom from Shame: Trauma, Forgiveness, and Healing from Sexual AbuseAún no hay calificaciones
- Unspeakable: Surviving My Childhood and Finding My VoiceDe EverandUnspeakable: Surviving My Childhood and Finding My VoiceCalificación: 4.5 de 5 estrellas4.5/5 (7)
- Girls Like Us: Fighting for a World Where Girls Are Not for Sale, an Activist Finds Her Calling and Heals HerselfDe EverandGirls Like Us: Fighting for a World Where Girls Are Not for Sale, an Activist Finds Her Calling and Heals HerselfCalificación: 4.5 de 5 estrellas4.5/5 (49)
- Scoundrel: How a Convicted Murderer Persuaded the Women Who Loved Him, the Conservative Establishment, and the Courts to Set Him FreeDe EverandScoundrel: How a Convicted Murderer Persuaded the Women Who Loved Him, the Conservative Establishment, and the Courts to Set Him FreeCalificación: 3.5 de 5 estrellas3.5/5 (19)
- Somebody's Daughter: Inside an International Prostitution RingDe EverandSomebody's Daughter: Inside an International Prostitution RingCalificación: 5 de 5 estrellas5/5 (3)