Documentos de Académico
Documentos de Profesional
Documentos de Cultura
24.amputations of The Foot and Ankle
Cargado por
steoeviciDescripción original:
Título original
Derechos de autor
Formatos disponibles
Compartir este documento
Compartir o incrustar documentos
¿Le pareció útil este documento?
¿Este contenido es inapropiado?
Denunciar este documentoCopyright:
Formatos disponibles
24.amputations of The Foot and Ankle
Cargado por
steoeviciCopyright:
Formatos disponibles
CHAPTER
24
Amputations of the Foot and Ankle
James W. Brodsky
GENERAL CONSIDERATIONS SURGICAL CONSIDERATIONS Tourniquets Soft Tissue Preservation Wound Closure Drains Skin Grafting and Flap Coverage
Vascular Reconstruction Determination of Amputation Level Other Factors Affecting Healing SPECIFIC AMPUTATION LEVELS AND TECHNIQUES (video clips 3 and 4) SUMMARY
Amputation of part or all of the foot is an ancient procedure, if not the oldest form of foot surgery, but surgeons often abhor foot amputations. Perhaps the reason is the repugnance of removing a body part, perhaps because amputation is seemingly so unaesthetic, or perhaps because amputation is seen, consciously or not, as an admission of failure, a form of surgical defeat. However, in the patient who has a foot that is no longer either viable or functional, an amputation is a positive procedure because it is the rst step on the road to restored or renewed function. The amputation is therefore the beginning of rehabilitation for these patients, many of whom have become debilitated both physically and emotionally in the battle to save part or all of a foot. In this process the functions and activities of normal daily life have been held hostage to the hopes and efforts to save the foot, often past the time of reasonable expectations for good function. To save a poorly functioning foot of marginal viability is to have won the battle and lost the war, because the goal
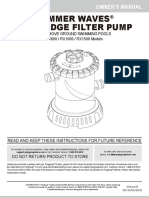
is to enhance the function and quality of life for the patient, not for the limb. Once a decision to amputate has been made, a number of challenges remain. These include selection of the proper level of amputation (Fig. 241), methods of foot salvage to maximize function, proper surgical technique, postoperative management, and footwear modication and the use of prostheses. The many causes of partial or complete foot amputation include the following: 1. Diabetes (many diabetic patients also have peripheral vascular disease) 2. Peripheral vascular disease (in the absence of diabetes) 3. Trauma (most often lawnmower injuries and motorcycle trauma) 4. Chronic infection (primarily osteomyelitis) 5. Tumors 6. Congenital abnormalities
1369
1370
PART VI
Diabetes
Choparts Symes
Transmetatarsal Metatarso-phalangeal disarticulation
Lisfrancs Toe amputation or disarticulation
Figure 241
Levels of partial foot amputation.
Amputation of part or all of the foot is correctly viewed as a procedure of last resort and reects the surgeons proper desire to save the foot. The term foot salvage emphasizes the contemporary shift from complete to partial foot amputations. The goal is to convert many of the procedures that in the past would have been below-knee amputations to partial foot amputations and, in the process, to convert these patients to users of modied footwear rather than users of prosthetic limbs.46
GENERAL CONSIDERATIONS
The goals of an amputation are fundamentally greater in the patient who requires ablative surgery as a result of trauma than the goals in patients requiring amputation for diabetic foot problems. The diabetic patient or the patient with insensitivity from any cause needs to achieve a plantigrade foot with stable healing of the wounds, and the lowest possible risk for future ulceration. The patient whose amputation is a result of trauma also needs an extremity that is not painful. This is compounded by an increased proclivity of traumatic amputations to develop symptomatic neuromas and complex regional pain syndrome (CRPS, reex sym-
pathetic dystrophy). The advantages and disadvantages, as always, are two sides of the same coin. The traumatic amputee is not subject to the same frequency of recurrent problems and multiple revisions of the amputation to a higher level (not to mention risk to the contralateral leg19) as a diabetic patient because the (presumably sensate) limb of the traumatic amputee has sufcient sensation to prevent neuropathic breakdown of the soft tissues. One of the major goals in amputation surgery of the foot is to salvage as much of the functioning foot as possible. The general principle holds true that preservation of a greater portion of the limb allows greater function. The classic experimental basis for limb preservation was documented in a study done at Rancho Los Amigos Hospital that showed increasing energy costs of walking, as evidenced by greater oxygen consumption, in patients who had higher levels of amputation.47 The two qualications of that principle are that the salvaged foot must achieve complete healing with a stable soft tissue envelope, and the foot must be sufciently plantigrade to be functional. Partial foot amputations (e.g., transmetatarsal or ray resections) are worthwhile because they allow the use of fairly normal shoes, often with only minor modications. However, a higher amputation level may be better for the patient and yield a more functional result
CHAPTER 24
Amputations of the Foot and Ankle
1371
if the patient becomes debilitated because of prolonged and unsuccessful treatment in an attempt to save a portion of the foot, for example, a toe or one metatarsal. In the course of achieving healing of the partial foot amputation, the patient is nonweight bearing, full time or intermittently, and the upper extremities are occupied with ambulation, thereby limiting the patients ability to participate in most activities of work and daily living. Thus the goal of foot salvage must be tempered by the functional result and the time required to achieve the healing. The patient is usually better served with a more proximal but denitive and healed amputation that allows walking and resumption of daily routines than if rendered incapacitated with protracted wound care in an attempt to save a portion of the foot that adds little to ultimate function. Although the conversion from below-knee amputation to more distal amputation is still an ongoing process with some of the surgical specialties, partial foot amputations have been clearly shown to result in superior function, greater mobility, better cosmesis, enhanced lifestyle, lower energy consumption, increased sensory input, better weight-bearing surface, and less distortion of body image than transtibial amputations.
In the case of below-knee amputations, it is reasonable and very often helpful to use a thigh tourniquet to improve visualization, especially for ligature of the vascular bundles. The tourniquet is released prior to wound closure to check for hemostasis.
Soft Tissue Preservation
The most important rst step in amputation surgery is aggressive debridement of infected and necrotic bone and soft tissue. This must be balanced by the need to preserve the maximum amount of viable skin and soft tissue, especially plantar aps, because they make the best soft tissue coverage of weight-bearing surfaces. When the amputation is done for gangrene, the initial and preliminary line of resection should be quite close, usually a few millimeters, from the edge of the gangrene, in order to save the most soft tissue. At the time of return to surgery for closure, if the edge proves not to be viable, it can be cut back farther at that time. Surprisingly, the skin is usually viable because the level of nonviability has already been demarcated. Taking a too-generous margin of skin often can force the surgeon to go to the next higher level of amputation. The surgeon should not hesitate to make irregular or asymmetric aps and then to reevaluate the pattern of closure once a bleeding edge has been obtained all around the wound. The surgeon must make the best use of the available soft tissue and is encouraged to use creative local aps. The principle is to make use of the areas of viable tissue that might not t the pattern of a standard ap for the level of amputation. For example, the pattern of locally viable tissue might allow one to swing a local ap medially to laterally instead of using the typical long plantar ap for closure of a transmetatarsal amputation. The innovative use of local tissue in such a situation often is the only way to achieve closure at that level. Otherwise, the patient has the disadvantage of requiring a more proximal amputation. This type of local ap is also preferable to a skin graft because it is more durable and more sensate. Classically, the ideal length of the ap is approximately half the width of its base. However, the real-life situation of patient care is not always ideal, and some allowance must be made for the vagaries of each case if it affords a potential advantage to the patient. Residual local aps often need to be thinned, especially where they form corners. This is true at all levels of amputation. As the excessively thick ap is folded over, it bunches up in the corner and pushes the skin edges away from each other. Thinning the ap excessively can disturb the vascularity of the skin edge; some residual thickness contributes to a natural eversion of the edges.
SURGICAL CONSIDERATIONS Tourniquets
Although the use of tourniquets in amputation surgery has often been proscribed in the past, the experimental basis for this prohibition is lacking. A controlled, randomized trial of tourniquet use in foot amputations in diabetic and dysvascular nondiabetic patients demonstrated no difference in healing rates between patients with tourniquets and those who did not have tourniquets applied.6 In this series the tourniquet was released once the amputated part was removed, before beginning the closure, to check for hemostasis and ap viability. Use of tourniquets requires three other considerations: the location, the type of tourniquet, and the presence of underlying vascular bypass grafts. For partial foot amputations, if a tourniquet is desired or needed, an Esmarch bandage just above the malleoli is safe and effective.5,6 For more proximal amputations, a thigh tourniquet is required and thus must be a pneumatic tourniquet. Although easy to use, thigh tourniquets can inhibit quadriceps function postoperatively, which may be a consideration in some patients. Surgeons are reluctant to place a tourniquet over this area in patients with vascular bypass grafts.
1372
PART VI
Diabetes
If doubt exists about the viability of an area, the area can be preserved and observed and then further debrided at the next session in the operating room. Especially with an infected wound, the patient might require two or three sessions in the surgical suite: the rst time for initial, aggressive debridement; the second time, if needed, for redebridement of residual areas of infection or necrosis after a period of intervening wound care; and denitive closure at that or a subsequent session. Occasionally it is necessary to expand the middle step to more than one secondary debridement. After the debridements, the wound is usually left open to allow drainage and wound care. Surgical redebridement at intervals augments wound care until the wound is clean or has good granulation. In many cases the focus of infection is sufciently distal or localized that the debridement and closure can be done in a single session (see the discussion of surgical treatment of infection in Chapters 23 and 35).
Wound Closure
The nal wound, especially in a partial amputation of the foot, must be fashioned to balance the length of preserved bone with the available soft tissue to cover it. Wound closure, and thus the ultimate length of the foot, is almost always a function of the amount, location, and shape of the remaining viable soft tissue. If there is deep infection of the bone, the overlying soft tissue is usually compromised by infection as well. Once both are resected to a level proximal to the infection, the bone length can be balanced to the soft tissue. In many cases it is necessary to sacrice an additional portion of the osseous structure to achieve this balance. With an infected diabetic foot, this can signify excision of additional uninfected metatarsals in order to achieve delayed primary closure of a partial forefoot or transmetatarsal amputation. In an example of a partial forefoot amputation, the metatarsal in question would have been partially exposed at surgery. With subsequent skin closure, the surgeon nds it impossible to completely cover the wound with the remaining viable skin and soft tissue, and skin grafting would not result in a stable closure. An example of a transmetatarsal amputation is a patient in whom the medial two or three rays have been partially resected for osteomyelitis and the remaining lateral rays create an insufcient platform for weight bearing. Resection of the uninfected rays allows a better balanced and more functional foot. Once a clean, granulating wound is achieved, whether the procedure is a diabetic or a posttraumatic amputation, the wound should be closed. Although primary closure cannot always be achieved, especially
in the dysvascular or diabetic patient, the surgeon should strive for primary closure of the amputation site. This can be either immediate primary closure at the time of resection or delayed primary closure at the second or third procedure in the surgical suite. This can be attained in the majority of cases. Failure to achieve primary or delayed primary closure in a large number of cases signies poor decision making. Leaving large gaping wounds to granulate inward as the main method of healing amputations, especially in diabetic patients, condemns the patient to an unnecessarily and very long recovery (Fig. 242). This technique often represents the surgeons failure to make a decision about the viability of the local tissue and the appropriate nal level of healing. It is more effective and far more cost-effective, not to mention less debilitating to the patient, to establish an assessment of the vascularity and healing potential of the partial foot amputation wound and do a denitive procedure with good, viable local closure. If needed, the limb should rst be revascularized by the vascular surgeon and then redebrided and eventually closed at the new level of viability. Allowing an entire amputation wound to granulate slowly is an extremely slow process. Large wounds that are left to granulate very often require skin grafting and produce an irregular scar or an invaginated skin surface. The process of wound contracture can be hindered by the shape of the wound and the amount of residual bone structure beneath. Delayed primary closure is valuable, even if it only achieves partial closure of the wound. It reduces the amount of coverage to be achieved and speeds healing. In such cases, the wound aps adhere over part of the wounds length, and a portion fails to close and continues to drain small amounts. This still reduces the morbidity because the residual wound that must be treated and
Figure 242 This wound was left open to granulate owing to infection, irregular contours, and nondenitive debridement. This was revised and closed primarily.
CHAPTER 24
Amputations of the Foot and Ankle
1373
that must granulate inward is still only a fraction of the original wounds size. I have advocated this technique previously.11,29 The validity of this concept has been reafrmed by the advent of negative pressure wound dressings.10,15,30,39 The technique does not work for every case, and it certainly cannot overcome inadequate debridement or inclusion of nonviable soft tissue. However, primary closure, even when partial, is a durable technique for maximizing foot salvage. A common pattern is adherence and closure of the two ends of the suture line, with a small dehiscence in the middle third. The sutures in the healing areas are usually left in place for a minimum of 4 to 6 weeks, occasionally longer while wound care continues on the central portion of the wound. This is an important consideration because the entire wound in a diabetic or dysvascular patient can take many months to granulate inward. If partial closure is achieved, the time to complete healing is greatly reduced. There are several possible explanations for a wound that does not appear ready for delayed primary closure. Debridement might have been inadequate, and nonviable tissue remains; the soft tissue aps might have inadequate vascularity; or the wound might have had insufcient time to begin granulating. Even if it is decided to cover the wound with a split-thickness skin graft, a good granulating base, or well-vascularized tissue (e.g., muscle), is necessary rst. In amputation closures, the skin edges are handled as little as possible. Forceps should be used on the subcutaneous and deeper layers, rather than on the skin edges. Flaps should be tested at closure by gently bringing them together manually. This should demonstrate an ability to close the wound without tension. If such a closure cannot be completed, more of the underlying bone must be resected to reduce the pressure on the aps. The stump should be palpated through the aps to make sure that no rough edges, sharp angles, or undesirable bony prominences remain. The balance of soft tissue to bone discussed earlier is most evident at closure because there should be no tension on the skin edges or suture line. The surgeon should inspect the skin for blanching as a sign of an overly tight closure. In diabetic amputations the sutures should be left in place an extended time, usually at least twice as long as in a nondiabetic patient. In most of these patients the nylon skin sutures, which are nonreactive, should be left in place a minimum of 4 weeks, and sometimes longer. It is not necessary to resect the cartilage from the exposed surfaces at the level of the amputation. Preservation of the cartilage, and thus of the underlying subchondral bone, can create a barrier to infection of the residual bone. The clearly dened line of the sub-
chondral bone makes it easier to follow the postoperative radiographs for changes such as erosion of the distal bone.
Drains
Drains are usually used at the time of the delayed primary closure. Some form of suction drain is preferable. The type depends on the surgeons judgment, the conguration of the wound, and the characteristics of the wound closure. Penrose drains, which typically exit through the closure and between the sutures, are discouraged. They tend to interfere with early adherence of the wound edges in that location and are less effective than a suction drain in reducing postoperative collection of uid or hematoma. Ideally, the drain should exit through a small separate stab wound.
Skin Grafting and Flap Coverage
Skin grafting is an acceptable technique for obtaining coverage (as distinguished from closure) of amputation wounds. Split-thickness grafting is somewhat more successful in traumatic amputations than in those done in insensitive diabetic feet. Because of the loss of protective sensation, primary closure with local soft tissue aps is still preferable in diabetic patients. Skin grafts often make the difference between salvage and loss of an amputation stump, but they have a higher rate of recurrent breakdown than local skin coverage. Free tissue transfer has been a valuable adjunct to limb salvage, especially in traumatic amputations of the foot. The greatest benet has been in obtaining coverage over wounds of the ankle, heel, and hindfoot. These areas have relatively little subcutaneous tissue, and the skin, especially in the hindfoot, is xed and immobile, which makes rotation of local aps difcult. Free tissue transfers are difcult, and they add time, expense, and morbidity to the patients recovery. Their use should thus be thoughtfully justied. In general, the technique is not often applicable to the forefoot and midfoot. However, when appropriately indicated for coverage of a soft tissue defect over the hindfoot or heel, a free tissue transfer has the potential to create a great difference in functional outcome. The dramatic effect is attributable to converting the patient who has no heel from a user of a prosthesis (e.g., Symes ankle disarticulation or below-knee amputee) to a user of a shoe.
Vascular Reconstruction
With an amputation in a diabetic or dysvascular limb, the skin edges should be checked once the nal aps
1374
PART VI
Diabetes
have been fashioned. If there is not at least a small amount of visible bleeding, the aps should probably be revised to a more proximal level. Typically the surgeon checks for the presence of punctate bleeding spots in the aps and especially along the skin edges. When the limb is dysvascular, vascular consultation should be obtained. Revascularization of the limb can be done through angioplasty, placement of a proximal stent, endarterectomy, proximal bypass, or distal bypass surgery. Regardless of the technique, revascularization is often the key to salvage of the foot. It is crucial to remember this and to work as a team with vascular surgeons. Bypass is the most common of these techniques. Balloon angioplasty is applicable primarily to discrete, well-localized (and usually proximal) occlusive lesions, which are relatively uncommon in diabetic patients and more common above the popliteal artery in nondiabetic vascular disease. In the nondiabetic patient, bypass usually takes the form of proximal bypass of a major occlusion at the iliac, femoral, or popliteal levels. In the dysvascular diabetic patient, similar proximal occlusions or stenoses occur and respond well to a vascular bypass. In addition, and very commonly, diffuse occlusions of the arteries distal to the trifurcation of the popliteal artery can occur in the lower part of the leg. Unlike in the nondiabetic patient, these are not discrete blockages but usually consist of atherosclerotic involvement diffusely through the vessel. Bypass done down to the level of the ankle may use in situ or reversed saphenous vein grafts. The emphasis should be on doing the revascularization before fashioning the nal amputation aps. Preferably, the nal level of amputation is determined once maximum tissue perfusion has been achieved.7 The customary surgical techniques described here are basic guidelines, not absolute requisites, for successful amputations. No matter what the conscientious surgeon does, some amputations will fail and will need to be revised to a higher level. If every amputation heals primarily, the surgeon may be doing some amputations at too proximal a level and not achieving enough salvaged cases from the feet. Often several procedures and revisions are needed before the nal result is obtained, and the revisions do not prejudice the quality of the ultimate result; rather, they make the attempt at foot salvage worthwhile.21,23,27 Healed amputations that result from revision procedures yield satisfactory results similar to those that heal after a single level of amputation. Once partial amputations of the foot heal, the reported rate of revision is as low as 10%, thus indicating that these function as denitive procedures. The surgeon uses imaging and laboratory data, clinical experience, and surgical judgment to select the level for partial foot amputation.
Determination of Amputation Level
A plethora of tests have been promulgated in the surgical and orthopaedic literature as the best method to determine the proper level of amputation. Most are based on statistical review of ultimate healing of the amputated limb and the correlation with predicted healing from the test. These procedures include arterial Doppler pressure measurements, uorescein angiography, transcutaneous oxygen tension measurements, and xenon clearance.12,34,37,50 The literature is replete with these reports, although all the studies examine levels of healing on the thigh and leg. Most of these studies do not address the question of the proper level of amputation within the foot, that is, the question of the correct level for a partial foot amputation procedure. For this reason, these studies are often difcult or impossible to apply to the decision-making process of foot salvage, which depends greatly on local wound factors of gangrene, infection, and general perfusion of the foot. Differences in vascularity between a transmetatarsal amputation and a Syme ankle disarticulation are at best difcult to determine on the basis of most noninvasive preoperative testing. Even when tests indicate differences, their reliability for differentiating levels of viability within the foot has not been clearly proved or widely accepted. Most of the studies on predictive tests for amputation healing levels have been aimed at assessing the segmental vascularity of the limb, that is, healing below the ankle, at the ankle, below the knee, or above the knee. None of the procedures has been demonstrated to have a clear hegemony in this battle to forecast healing accurately, at least not in the arena of widespread clinical practice. Each of these procedures has clear advantages, and a few of these characteristics are mentioned here, although this is by no means an exhaustive review of this broad subject. The most commonly used and widely available test is the arterial Doppler ultrasound. This is most useful as a guideline to general levels of perfusion and is the best initial screening test to determine whether the patient needs a vascular surgery consultation and an arteriogram. The Doppler ultrasound is painless, quick, and inexpensive and does not require extensive instrumentation. As discussed in the section on vascular evaluation in Chapter 23, the pulse-volume recordings (waveforms) are reliable indicators of perfusion, but ratios of ankle pressures to arm pressures can be unreliable, especially in the diabetic patient with noncompliant, calcied vessels that give falsely elevated pressures. For healing of distal amputations, the most reliable measures are toe pressures. A forefoot amputation is likely to heal with a toe pressure of
CHAPTER 24
Amputations of the Foot and Ankle
1375
40 mm Hg or greater. Distal wound healing in the presence of toe pressures between 30 and 40 mm Hg is possible but less predictable.3 Some authors advocate transcutaneous oxygen measurements. These measurements are clearly much more cumbersome to perform than Doppler studies. The readings must be obtained in an environment of controlled temperature because they are temperature dependent, and they are time consuming to perform. On a practical level, an adequate number of readings cannot be done efciently without multiple simultaneous probes. No equivalent to Doppler toe pressures exists; thus this technique does not offer information about healing of the most distal procedures. Recent studies have questioned the reliability of transcutaneous oxygen measurements. 41 The real question is to what degree the surgeon nds a correlation of test results with wound edge bleeding at surgery and with the healing rate of amputation wounds in that particular institution.
ing healing. Published measures of this are the total lymphocyte count, which should be greater than 1500/L; serum albumin 3.5 g/dL or greater; total protein 6.2 g/dL or higher; and hemoglobin greater than 11 g/dL.
SPECIFIC AMPUTATION LEVELS AND TECHNIQUES
AMPUTATION OF THE DISTAL TOE AND NAIL The terminal Syme amputation, which has been described for severe posttraumatic nail deformity, onychomycosis, or recurrent infection of the great toenail, can be used for the same problems in a lesser toe as well. The key is to remove sufcient bone to allow closure without tension. Surgical Technique 1. The nail plate is removed (Fig. 243A). An elliptical incision is centered over the distal aspect of the distal phalanx encircling the toenail plate. The incision must extend sufciently proximally to include all of the proxi-
Other Factors Affecting Healing
Other factors that affect healing include edema in the local tissues, systemic disease, and nutritional factors. Systemic factors include glycemic control in diabetic patients or vasculitis in patients with inammatory arthritides. As noted in Chapter 23, simple indices of nutritional status can have a predictive value for wound healing after amputation.13 Of course, the adequacy of nutritional status is important to achiev-
Figure 243 Terminal Symes amputation. A, The nail plate is removed. B, An elliptic incision is centered over the distal aspect of the distal phalanx encircling the toenail plate. C, The dorsal soft tissue, nail plate, and eponychial folds are excised as a single fullthickness mass. D, The distal phalanx is transected with bone-cutting forceps or a small saw and the distal fragment is removed. E, A single interrupted layer of sutures is used to loosely approximate and evert the skin edges.
B A
1376
PART VI
Diabetes
2.
3.
4. 5.
6.
mal and lateral eponychial folds to prevent partial nail regrowth (Fig. 243B). The dorsal soft tissue, nail plate, and eponychial folds are excised as a single full-thickness mass down to the bone, to expose the distal phalanx (Fig. 243C). The distal phalanx is transected with a bonecutting forceps or small saw and the distal fragment is removed (Fig. 243D). Approximately one third to one half the phalanx is removed, depending on the amount of soft tissue for coverage. The skin ap is shaped to minimize medial and lateral dog ears, although the tissue will shrink and reshape after healing. A single interrupted layer of sutures is used to loosely approximate and evert the skin edges. A loose skin closure usually allows adequate drainage and usually obviates the need for a drain (Fig. 243E). A gauze-and-tape dressing is applied.
Sutures
Minimum 1 cm bone
Postoperative Care Skin sutures are removed 4 to 8 weeks after surgery. Early suture removal is avoided because it can lead to dehiscence, especially because the ap is thick and stiff. Pitfalls and Complications Shaping of the excised ellipse of tissue is important; a bulbous end can form, and although it usually shrinks to some degree, aps should be sculpted to minimize this. The main complication is dehiscence from a tight closure caused by insufcient resection of bone. In diabetic patients or nondiabetic dysvascular patients, preoperative vascular studies should be done to screen for healing potential of this most distal segment.
Figure 244 Preservation of at least 1 cm of the base of the proximal phalanx in amputations of the hallux is desirable to maximize the weight-bearing function of the rst metatarsal. This patient has two thirds of the proximal phalanx preserved.
intuitive and scientic. The benets of preserving the base of the phalanx for the subsequent gait of the patient and the pattern of pressure under the foot have been demonstrated in plantar pressure studies with the pedobarograph. The intuitive basis is that by saving the base of the phalanx, the attachments and thus the functions of the plantar fascia and exor hallucis brevis tendon are preserved, at least partially. The independent plantar exion mechanism of the rst ray is not entirely lost, and some of the weight-bearing function of the rst ray may be preserved, possibly reducing the transfer of pressure to the second and third metatarsal heads. Surgical Technique
AMPUTATION OF THE GREAT TOE THROUGH THE PROXIMAL PHALANX BASE Although it is technically easier to amputate the great toe through a metatarsophalangeal (MTP) disarticulation, there are potential advantages to saving the base of the proximal phalanx. The minimum length of the base to save is about 1 cm (Fig. 244). This recommendation is both
1. A curvilinear skin incision is used to encircle the dysvascular or infected area and to excise nonviable tissue. 2. The surgeon determines the length of the aps required for closure of the wound. At the base of the phalanx, or at the MTP joint, viable aps must be present to the level of the distal part of the proximal phalanx. 3. Often, sufcient skin is present on the dorsoplantar aspect or mediolateral aspect of the hallux to enable the development of sh
CHAPTER 24
Amputations of the Foot and Ankle
1377
Figure 245 Racquet-type incision for toe amputation. A, Outline of continuous incision. B, After disarticulation. C, Closure.
4.
5.
6. 7.
mouth aps (an alternative is a racket-type incision) (Fig. 245). A power saw is used to transect the proximal phalanx at its base, leaving a minimum of 1 cm length. Rough edges are beveled with a rongeur. If the base of the phalanx has been preserved, at least one of the sesamoids must be saved because the sesamoid complex attachment to the phalangeal base is the key to the function of the phalanx if it is to aid in maintaining some weight-bearing function of the rst metatarsal. The aps are approximated with fullthickness, interrupted sutures of a nonreactive monolament. A gauze dressing is applied.
METATARSOPHALANGEAL DISARTICULATION OF THE GREAT TOE In some cases, it is preferable to amputate through the MTP joint. There are several important technical points. It is not necessary to remove the cartilage from the metatarsal head, as noted in the section on wound closure. The most important technical point is that the aps must be viable (bleeding edges, no residual necrotic tissue) and must be easily closed without tension on the skin edges. It is surprising how distal the aps must be in order to achieve closure without tension. In general, the length of the aps must be at a minimum, equal to half the length of the proximal phalanx.
Once the proximal phalanx has been resected, and prior to closure, the sesamoid complex should be inspected. As with most distal foot amputations, the extensor and exor tendons are resected proximal to the level of closure. The exor hallucis longus passes between the sesamoids in a tight sheath. In many cases of disarticulation of the hallux, the sesamoids retract. However, if they do not, or if the sesamoids are enlarged and arthritic, postoperatively they can create plantar pressure under the rst metatarsal, constituting a risk for ulceration in the neuropathic patient. The conjoined tendons of the sesamoid complex are relatively avascular, and the thickness can impede mobility of the plantar ap during closure. For these reasons, sesamoidectomy is often a necessary component of MTP disarticulation. This can take the form of excision of the medial sesamoid only, or of the entire complex of both sesamoids with the cradle of conjoined tendons. It is not typically necessary to resect the plantar crista of the rst metatarsal head. Postoperative Care Routine dressing changes are continued until adequate healing has occurred. In concept, it would seem preferable not to allow weightbearing postoperatively in order to protect the wound and the suture line from shearing forces that would pull the wound apart. In reality, many patients are not physically able to sustain nonweight bearing for the reasons elaborated in Chapter 23. A compromise is to allow weight bearing on the hindfoot only, but this is more difcult to achieve than it appears. The use of
1378
PART VI
Diabetes
AMPUTATION OF THE LESSER TOES Amputation of the lesser toes can be done as a disarticulation or as a resection through bone. If a toe requires amputation because of ischemia, necrosis, or circumscribed distal osteomyelitis, partial amputation is a reasonable alternative, provided that adequate perfusion exists to support healing. The advantage of this amputation over disarticulation at the MTP joint is that the residual partial toe serves to maintain its space and block migration of the two adjacent toes toward each other into the gap created by the absent digit (Fig. 247). Surgical Technique A similar surgical approach is used for resection of the various lesser toes as for the great toe. Although preservation of the base of the phalanx in the lesser toes probably produces the same mechanical advantage, it is less important than in the hallux. Regardless of whether the amputation is done distally at the level of the phalanx or as a disarticulation of the entire toe at the MTP joint, the types of closures are the same. The most important point to remember is that the two common types of aps are side-toside (sh mouth) aps and racquet aps. Fish mouth aps can be fashioned either as medial and lateral aps or as dorsal and plantar aps. The racquet incision is the easiest to use, and the surgeon must decide where to place the handle of the racquet, that is, the proximal longitudinal extension of the loop. It is most easily placed along the dorsum of the ray between the
Figure 246 amputations.
Molded insole for healed partial forefoot
partial shoes that allow the forefoot to hang over the distal edge of the shoe increases the pressure on the heel and hindfoot. Sutures are removed 4 to 8 weeks after surgery. Early suture removal should be avoided because wound dehiscence may occur. Once a great toe has been amputated, a custom-molded ller in the shoe helps to compensate for and diminish sliding of the foot inside the shoe (Fig. 246).14 Pitfalls and Complications The most common short-term complication of hallux amputation is poor wound healing, often because of inadequate perfusion at the amputation level. The most common long-term complication is the gradual migration of the second toe into varus and hyperextension at the MTP joint. In the diabetic patient with neuropathy, this can lead to pressure ulceration over the proximal or distal interphalangeal joints. As the extension deformity worsens, another ulceration can develop under the second metatarsal. In diabetic patients, an occasional problem is a recurrent ulceration or pressure area near or on the rst metatarsal. Once healing of the hallux amputation has been achieved, the patient needs to be tted with an accommodative insole to balance the weight-bearing pressure over the forefoot.
Figure 247 Partial toe amputation. The residual portion of the digit blocks migration of the adjacent toes.
CHAPTER 24
Amputations of the Foot and Ankle
1379
zones of the two neurovascular bundles to the digit (see Fig. 245). There are two proximal extensions in the sh mouth aps. If the aps are placed dorsally and plantarly, the extensions run over the neurovascular structures, making medial and lateral aps preferable (Fig. 248). In a few cases, disarticulation of all the toes at the MTP joints is a viable alternative, primarily for trauma, such as a lawnmower injury to all the toes. If reasonable soft tissue coverage can be obtained, the foot can be extremely functional. The preservation of length makes footwear much easier to t than with a transmetatarsal amputation because a low quarter shoe will stay on the foot. If a patient has had more than one toe amputated at different times, as often occurs in diabetic patients, it is important not to leave the patient with just one or two remaining toes. These are condemned to experience pressure and ulceration and then to require amputation, because the pressure of footwear and walking will be concentrated there. At this point it is best to remove all the toes, through either MTP disarticulation or transmetatarsal amputation, to even out the distal forefoot. Aftercare In the immediate postoperative period the patient is kept in a bulky bandage and a surgical shoe. Splints are required if a concomitant Achilles tendon lengthening or other hindfoot procedure has been done. The surgical shoe or other protective footwear continues to be worn until the soft tissue healing is complete, both to prevent pressure on the wound by the shoe and to allow dressing changes. Toe separators, made of soft foam or Plastizote, help to retard drift of the remaining toes
into the defect made by the amputated digit. If the patient requires a molded insole, the toe separator can be built into it, but it is usually easier to keep it separate. Pitfalls and Complications The most common complications are related to inadequate balance of soft tissue and bone. This leads to dehiscence of wounds closed under tension. Other complications, as mentioned earlier, include drift of the adjacent toes toward the defect created by the missing digit. This can be retarded by the use of a toe separator soft pad made of Plastizote or similar materials worn inside the sock or stocking. In some cases, resection of the distal second or third metatarsal at the time of disarticulation of the toe allows immediate narrowing of the foot and closure of the gap between the digits (see following discussion of ray amputations). The drift of the lesser toes is seen most often after amputation of the second toe. The gap closes more naturally and with fewer problems after amputation of the fourth toe because of the greater mobility of the fourth metatarsal and the natural varus of the fth toe. Disarticulation of the fth toe at the MTP joint can leave the fth metatarsal head exposed to pressure of weight bearing, and sometimes it needs to be resected. A late deformity of a partial toe amputation is dorsal elevation of the stump caused by a hyperextension contracture at the MTP joint. In the lesser toes, this requires resection of the toe remnant back to the MTP joint or release of the extensor tendons and sectioning of the capsule of the MTP joint on three sides (medially, laterally, and dorsally).
Side-to-side flaps
Dorsal-plantar flaps
Racquet-type incision
Bone resection proximal to or at level of base of flaps
Figure 248 Types of incisions and aps for amputation of the lesser toes. A and B are sh-mouth closures. A, Side-to-side or medial and lateral aps. B, Dorsal and plantar aps. C, Racquet-type incision.
1380
PART VI
Diabetes
RAY AMPUTATION AND PARTIAL FOREFOOT AMPUTATION Amputation of a toe with all or part of its corresponding metatarsal is the denition of a ray amputation. These are more common than any other amputation of the foot except simple toe amputations. They are durable and, once they are healed, are relatively easy to t in shoes with minor modications and a molded insole. Narrowing of the foot can create problems of increased pressure under the forefoot or side-to-side movement within the shoe, but this usually can be accommodated by the use of the insole. The preservation of foot length is often an advantage because the longer forefoot makes it easier to keep on a shoe. Ray amputations are typically used to treat trauma in healthy patients as well as infection and gangrene in the dysvascular and diabetic populations (Fig. 249).
Border Ray Resection The easiest single rays to amputate are the border rays, that is, the rst and fth. Straight medial and lateral incisions are used, respectively. If only a small amount of the distal metatarsal needs to be resected, the distal end of the incision may loop around the base of the digit (the racquet). When possible, a longer plantar ap allows for an easier closure when the procedure involves the border of the foot. First-ray and fth-ray amputations are successful in preservation of foot length. Fifth-ray amputations are the most commonly successful ray amputation. Despite some controversy in the past, rst-ray amputations can function extremely well with a molded insole in the shoe that supports the medial border of the foot and includes a ller for the absent ray. Specic surgical techniques in partial forefoot amputation can vary greatly. Surgical incisions and osseous resections must be tailored to the individual problem area of infection, the magnitude of soft tissue necrosis, and the extent of osteomyelitis. Care must be taken to save some of the skin that is over the digit itself, if possible, and always to save more skin than would seem necessary. It is obviously easy to trim away excess skin, but insufcient soft tissue for closure leads to closure under tension, dehiscence, or wound necrosis (see Fig. 242). Failure to save all possible viable skin and soft tissue is the most common error of the surgeon inexperienced in amputation surgery. A llet ap can be created from the toe by removing the bone subperiosteally and preserving the full thickness of the soft tissue, which is then turned proximally to cover a defect and then trimmed appropriately (Figs. 2410 and 2411). Fillet aps can be done most easily on border rays. Central Ray Resection Single ray amputation of one of the three central rays (second, third, and fourth) is less familiar to most surgeons, and it is less often indicated than resection of the border rays. The primary technical challenge is the approximation of the relatively immobile soft tissue aps. Often the gap created by the absent ray closes without much difculty when the incision is closed. In some cases the defect allows the two adjacent toes to drift toward the amputated ray, as occurs
Dorsal skin Plantar
Level of bone resection
Figure 249 Partial foot amputations. The level of bone resection must be proximal to the level of viable soft tissue to achieve closure without tension on the aps. Satisfactory healing depends on this balance. Shading indicates amputated area.
CHAPTER 24
Amputations of the Foot and Ankle
1381
Closure can be facilitated by more proximal resection of the central metatarsal, which allows greater narrowing of the foot. It is advisable not to disarticulate the base of the metatarsal because this will destabilize the midfoot, leading to pain in the traumatic amputee and often to a Charcot neuropathic midfoot breakdown in the insensitive limb. Multiple Ray Resections: Partial Forefoot Amputation Partial forefoot amputations involve removal of two or occasionally three rays from the medial or lateral side of the foot. This is probably more successful in trauma patients but occurs more often in diabetic patients because more amputations are done because of diabetes than any other cause in our population (Fig. 2413A and B). In most instances, once it becomes necessary to amputate three rays, it is easier and yields a more predictably good result to perform a transmetatarsal amputation instead. On the whole, partial forefoot amputations of the lateral side fare better than those on the medial side of the foot, although there are successful examples of both even in diabetic and dysvascular patients. Loss of the rst ray results in an effective foot less often because the foot does not balance as well, and transferred pressure under the lesser metatarsals leads to further ulcerations. Forefoot, transmetatarsal, and Choparts amputations are the most common procedures in which the surgeon may want to use creative aps. This signies using viable local tissue that is available to close the wound even if it does not conform with the ideal ap placement or shape. The goal is to achieve primary closure over the maximum length of bone while still using durable local tissues, especially if this includes viable plantar skin (Fig. 2414A to C). Aftercare Proper footwear for the healed partial forefoot amputation is critical (see Fig. 246). The shoe must have additional width and depth in the toe box to accommodate the essential insole. A ller should be built as a part of the insole to block side-to-side motion of the remaining narrow forefoot (i.e., prevent the windshieldwiper motion that can occur with walking).
Figure 2411 Healed ap.
Figure 2410 The great toe soft tissue has been turned proximally to cover a defect over the rst metatarsal.
in a simple toe disarticulation at the MTP joint. The key to successful central ray amputations in diabetic and dysvascular patients, in particular, is to incise the skin and soft tissue that is being saved right at the edge of necrosis and infection, in other words, to save maximum soft tissue, including skin of the digit (Fig. 2412A to D).
1382
PART VI
Diabetes
Figure 2412 A, Plantar ulcer. B, Plantar ulcer is now draining dorsally as well, indicating a deep web-space abscess. C, Foot salvage by web-splitting incision from mid dorsum to mid plantar surface. D, Excision of central metatarsal allowed delayed primary closure.
Deformity of the remaining toes is common and takes the form of clawing as well as medial or lateral drift toward the absent rays. Footwear also must accommodate these problems. In some cases it is necessary to correct these secondary toe deformities surgically subsequent to the amputation (Fig. 2415). Pitfalls and Complications The two main complications of the resection of one or more rays are delayed or poor wound healing and a functionally compromised residual foot. The latter problem is that the foot bears weight unevenly, and recurrent pressure ulceration occurs under the residual metatarsal heads (Fig. 2416). In both cases, the best salvage is revision to a more proximal level, usually a transmetatarsal amputation. In the insensitive (usually diabetic) patient, another sequela can be the
development of Charcots midfoot joints. The midfoot collapses and produces a secondary deformity. This cannot be prevented, but it can be retarded by preserving the bases of the metatarsals whenever possible. With a rst-ray amputation, an additional point is preservation of the entire attachment of the tibialis anterior tendon. In cases that require resection of the base of the rst metatarsal, the insertion of the anterior tibial tendon should be reattached proximally to the cuneiforms. This can be done through a tunnel in the bone, but it is easier to make a bed in the cancellous bone and attach the tendon with a bone anchor (Fig. 2417). The same is true for resection of the base of the fth metatarsal, namely, that the peroneus brevis tendon should be reinserted proximally if possible.
CHAPTER 24
Amputations of the Foot and Ankle
1383
Figure 2413 Example of lateral partial forefoot amputation. A, Dorsal view. B, Plantar view.
Figure 2414 A, Partial forefoot amputation for abscess and osteomyelitis. B, The maximum amount of soft tissue has been preserved, right up to the edge of viable tissue, to achieve closure. C, Healed wound. Patient resumed her original job in the mailroom.
1384
PART VI
Diabetes
Figure 2417 rior tendon.
Bone anchor for replantation of tibialis ante-
TRANSMETATARSAL AMPUTATION Transmetatarsal amputation is a sturdy, practical solution to severe gangrene, infection, or tissue loss in the forefoot.32 It is technically easy to perform and has a critical advantage over more proximal amputations because the insertions of the tibialis anterior and peroneus brevis tendons are preserved (video clip 4). This is important for active dorsiexion in walking, and it serves to counteract the pull of the triceps surae, which almost always produces an equinus contracture when unopposed or even unbalanced. Often concomitant lengthening of the Achilles tendon is necessary, with or without posterior ankle and subtalar joint capsulotomies, for an equinus contracture that has developed over a long period of nonweight bearing before the amputation. Subtle equinus, often difcult to recognize, is a cause of failure of this and other partial foot amputations. The surgeon should be sensitized to look for this problem in every patient before and after partial foot amputation. Based on studies of the effect of Achilles tendon lengthening in the treatment of diabetic ulcers, routine lengthening of either the gastrocnemius or Achilles tendon at the time of transmetatarsal and midfoot amputations appears to lower the risk of subsequent ulceration in neuropathic patients.35 The length of the transmetatarsal amputation can vary considerably, depending on the amount of soft tissue and the length of bone
Figure 2415
Molded insole for partial foot amputations.
Figure 2416 Recurrent ulceration after a partial forefoot amputation due to transfer of pressure to the remaining rays. The patient required a transmetatarsal amputation.
CHAPTER 24
Amputations of the Foot and Ankle
1385
that can be retained. Longer stumps have the advantage of holding onto a shoe better, but a short stump that heals primarily is better than a longer one that fails to heal or must be left open to granulate. Whenever possible, it is worthwhile to preserve all ve metatarsal bases. The traumatic amputee has better balance of the midfoot. In the diabetic patient with neuropathy, removal of one or more metatarsal bases can increase the risk of Charcot breakdown of the midfoot. This risk still exists after any partial foot amputation in a patient with severe neuropathy, even when all the bases of the metatarsals have been retained. Most patients with transmetatarsal amputations can be t in off-the-shelf footwear or at most a high-top shoe because of its additional lacing. The shoes generally need to have either lace-up closures or hook-and-loop (Velcro) closures. The shoe should have additional depth for a dual-density molded insole, to which is attached a block or toe ller that holds the shoe in the area of the missing forefoot (Fig. 24 20). Pitfalls and Complications The most common complication of transmetatarsal amputation is development of recurrent and recalcitrant ulceration on the stump. This can be caused by the plantar projection of one of the residual metatarsals or by new bone formation at the distal metatarsal, requiring resection of the prominence.4 Most often, ulcerations occur on the distal edge of the stump and result from an equinus contracture at the ankle and to some extent the transverse tarsal (Chopart) joint. Treatment consists of Achilles tendon lengthening (occasionally augmented with caspsulotomies of the ankle and subtalar joints), resection of the bony prominence, and debridement or excision of the ulcer. Postoperative treatment requires immobilization in a cast, preferably in slight dorsiexion, because of the risk of recurrent deformity. When skin grafting is necessary to supplement wound closure, which occurs rarely, it can be used on the dorsum of the foot. On the plantar surface it is much less successful, and careful consideration should be given to revising to a more proximal level if major skin loss has occurred on the sole.
LISFRANCS AMPUTATION (TARSOMETATARSAL DISARTICULATION) Lisfrancs amputation (tarsometatarsal disarticulation) and Lisfranc himself are historic. Lisfrancs writings preceded the popularization of transmetatarsal amputations by more than two centuries. Lisfranc, a surgeon in Napoleons army, is remembered most often nowadays for the application of his name to the anatomic complex of the tarsometatarsal region, and injuries thereof, although he described amputation, not fractures and dislocations, at this level. This reects, just as the eponymous Syme amputation, the high mortality associated with amputations that traversed bone in the era prior to antisepsis. Thus the most successful amputations were disarticulations. The recommended technique for Lisfrancs amputation is essentially that of the transmetatarsal amputation, including Achilles or gastrocnemius lengthening and reimplantation of the tibialis anterior and peroneus brevis tendons. Surgical Technique (Figs. 2418 and 2419) 1. The proposed skin incision is marked preoperatively. 2. The skin incision, as in all amputations of the foot, is selected by the level of viable skin and soft tissue The incision is curved gently proximally in a medial-to-lateral direction to match the length of the metatarsals. 3. A full-thickness ap is developed dorsally down to the metatarsals. 4. The ap from the plantar surface is typically made longer so that it wraps dorsally around the resected ends of the metatarsals. Although this is not always possible, it is desirable. The use of local dorsal skin is still superior to split-thickness skin grafting and should be used if the plantar skin is insufcient. 5. The tendons are cut back to the proximal edge of the wound. 6. The metatarsals are resected with a small power saw. 7. The bones are beveled in a direction from dorsaldistal to plantarproximal to prevent a sharp plantar edge on the bone that can lead to later pain or ulceration. The metatarsals are cut in a cascade of length: each successively lateral metatarsal is cut
1386
PART VI
Diabetes
Figure 2418 Surgical technique for transmetatarsal amputation. A, Plantar skin incision. B, Metatarsals divided about 15 degrees from the transverse axis. C, Soft tissue divided from the metatarsal necks and heads. D, Toes divided from the plantar ap. E, Tendons drawn down and divided. F, Closure completed by bringing posterior ap dorsally.
Plantar
Incision
Dorsal
Plantar flap
Metatarsal base Lateral view
Cascade of length
Figure 2419
Incisions and level of bone resection for transmetatarsal amputation.
CHAPTER 24
Amputations of the Foot and Ankle
1387
8.
9.
10.
11.
12.
approximately 2 to 3 mm shorter than the metatarsal immediately medial to it. The fth metatarsal is at a greater increment compared to the fourth metatarsal because it tends to produce late effects of plantar pressure, presumably because it is the most mobile of all the metatarsals. Once the bones have been cut, the amputated forefoot is divided from the plantar ap by cutting from proximal to distal just under the bones down to the plantar skin edge. The plantar ap needs to be thinned to achieve closure without tension. The skin is preserved for a tension-free closure, and the plantar intrinsic muscles, plantar plates, and subcutaneous tissue are beveled from proximal to distal. Smooth, continuous surfaces are created to prevent multiple tags and tails of devascularized tissue. Excessive or uneven planing of the plantar ap can adversely affect the aps viability. The aps tend to bulge at the medial and lateral edges in particular. Closure in diabetic patients is done in a single layer with interrupted nonabsorbable sutures. In an infected foot, presuming that the infected area has been ablated, primary closure is still attempted, usually over a suction drain. The foot is carefully checked for an equinus contracture, with the knee both extended and bent. Appropriate lengthening of the Achilles tendon or the gastrocnemius musculotendinous juncture (modied Strayer procedure) is performed.
13. A compression dressing is applied. A carefully padded posterior splint is applied with the ankle held in a neutral to mildly dorsiexed position. The splint is used to maintain neutral to slight dorsiexion if tendon lengthening is performed. Postoperative Care Sutures in diabetic patients are left in place a minimum of 4 weeks, but they are often kept twice this long. The patient is kept nonweight bearing until wound healing is certain. A postoperative cast may be used after the rst week or so, depending on the wound healing and whether a lengthening of the Achilles or gastrocnemius was performed.
CHOPARTS AMPUTATION This disarticulation through Choparts joint, that is, the transtarsal joints of the talonavicular and calcaneocuboid joints combined, had fallen into disfavor but has been repopularized by Jacobs and other authors in recent years.8,9,28,33,38 Choparts amputation has great and distinct advantages over both the Syme procedure and the below-knee amputation. First, it is technically much easier to do than a Syme amputation. Second, when the patient is tted postoperatively with an ankle-foot orthosis (AFO), the patient can wear a shoe rather than the knee-high prosthesis required both by Symes and below-knee amputations (Fig. 2421A to E). Third, Choparts amputation does not produce as much shortening of the limb. Fourth, as with Symes amputation, Choparts procedure is preferable to a below-knee amputation because its distal surface is covered by the tough weight-bearing skin of the heel: it is a distally weight-bearing amputation. There are numerous possible variations of the Chopart amputation for which the surgical technique is equivalent and that function equally well. These are amputations in which the level of disarticulation may pass through the naviculocuneiform joints medially or the cuboidmetatarsal joints laterally.
Figure 2420 amputation.
Shoe insole with toe ller for transmetatarsal
1388
PART VI
Diabetes
D
Figure 2421 Bilateral distal gangrene due to embolism. A, Left foot with a more proximal level of gangrene. B, Right foot with gangrene involving the toes. C, Plantar views. D, Right transmetatarsal amputation and left Choparts amputation. E, A shoe insole with a toe ller on the right and an anklefoot orthosis (AFO) with ller on the left allow the patient to wear low-counter laced shoes.
Choparts amputation can fail because of late equinus deformities that develop as a result of the unbalanced or unopposed pull of the Achilles tendon. Therefore it is necessary to plan for muscle balancing as an integral part of this procedure. The surgeon must completely divide the Achilles tendon at the time of the amputation. Simply lengthening is inadequate because the tendency for recurrence of equinus is so great. Although recurrence may be diminished by resection of a segment of the Achilles
tendon, reestablishing anterior tendon function is probably more important. Second, the tendons of dorsiexion (anterior tibial, peroneus brevis) should be transferred proximally to the talus and anterior process of the calcaneus, respectively, to provide a dynamic force to oppose equinus. Once the ankle is healed, the patient must be tted into a polypropylene AFO, lined with cushioning foam. Although Choparts amputation has several advantages over Symes amputation, the indica-
CHAPTER 24
Amputations of the Foot and Ankle
1389
tions for its use are limited. Many patients who have an insufcient amount of viable soft tissue for a transmetatarsal amputation do not have enough for Choparts amputation and require either a Syme or a below-knee amputation. Surgical Technique 1. The skin incision is marked preoperatively. 2. The aps are created dorsally and plantarly if possible; otherwise, available tissue is used. The surgeon takes care to resect the soft tissue sufciently distal to the level of the disarticulation while remembering that the cross section of the foot at this level is wide (Fig. 2422A and B; see Fig. 22-1). 3. The skin is retracted and the resection is carried down directly through the soft tissue,
again leaving sufcient soft tissue to close over the amputation area. 4. The extensor digitorum longus tendons are severed and allowed to retract. The anterior tibial and peroneus brevis tendons are traced out to their most distal insertions, dissected out, and preserved. 5. Choparts joint is located. The dorsal and plantar ligaments of the calcaneocuboid and talonavicular joints are released (Fig. 2422C and D). 6. The Achilles tenotomy or tenectomy is performed to prevent the development of an equinus contracture. If the latter is performed, a separate posteromedial incision is made, developing full-thickness aps from skin to paratenon. A 2- to 3-cm segment of the tendon is excised and the wound is closed.
Tibialis anterior tendon
Peroneus brevis tendon
Figure 2422 Choparts amputation. A, Incisions, lateral view of dorsal and plantar aps. B, Dorsal view of incision. C and D, Flaps retracted after resection of distal foot. E, Transfer of tibialis anterior tendon through tunnel in neck of talus. Peroneus brevis tendon transferred into anterior calcaneus. F, After closure of incisions.
1390
PART VI
Diabetes
7. The anterior tibial and peroneus brevis tendons are transferred into the neck of the talus and the anterior process of the calcaneus, respectively (Fig. 2422E). 8. A soft compression dressing is applied, followed by either well-molded splints or a postoperative cast to hold the ankle in a slightly dorsiexed position. Postoperative Care The patient is maintained in a postoperative splint or cast that is changed intermittently to monitor wound healing. Sutures are removed 4 to 8 weeks after surgery depending on wound healing. Early suture removal should he avoided to prevent wound dehiscence. The patient is kept nonweight bearing during the healing process. An AFO with a built-in molded insole is tted after completion of healing to stabilize the ankle joint and to assist with ambulation by providing a rigid level within the shoe for progression of weight transfer from heel to toe. The distal part of the foot plate of the AFO should have a ller attached of molded foam material to hold the residual foot and prevent collapse of the distal part of the shoe. The shoe should be modied to have a rigid sole with a roller or rocker plantar surface in order to reduce pressure on the distal surface of the stump. Pitfalls and Complications The primary surgical pitfall in the Chopart amputation is failure to fashion the aps properly for coverage. Although it is seldom a problem to use irregular aps or aps based to one side (as a result of the limited available tissue), the problem is that this proximal part of the foot has a wide cross-sectional area. The length of the aps must be proportionate to cover this, and the surgeon can easily err in making this judgment. The primary technical error is failure to rebalance the extensor tendons by transferring the anterior tibial and peroneus brevis tendons into the hindfoot. The primary complication is the development of an equinus contracture leading to recalcitrant ulcerations and osteomyelitis. As with other amputations, poor soft tissue healing is the other major complication.
PARTIAL CALCANECTOMY Partial calcanectomy can be considered a form of below-knee amputation, and some authors classify it as such because it is an amputation of the back of the foot rather than the front.43 Technique and indications are discussed in Chapter 23. Partial calcanectomy is a method of salvaging the foot by removing the nonviable portion. A few case reports2,18,48 and several substantial series of patients12,24,43,49 indicate good results with this technique as an alternative to below-knee amputation for salvage of the foot with calcaneal osteomyelitis. As with other amputations, it requires special postoperative orthotic management, in this case in the form of a foam-lined posterior-shell AFO.
SYMES AMPUTATION The Syme amputation, or ankle disarticulation, is named for James Syme, professor of clinical surgery at the University of Edinburgh, who rst described it in 1843. Invented in the era before antisepsis, antibiotics, or anesthesia,20 the great advantage of this amputation was that it did not have the 25% to 50% mortality of the belowknee amputation, which often became infected from contamination in a large wound that contained the transected medullary cavities of the tibia and bula. Although advances in medicine have negated many of the advantages of the rst century of use of this procedure, it still retains the other major advantage originally ascribed to it: in Symes words, a stump of greater comfort and utility when compared with the below-knee amputation. This advantage derives from the residual limbs being longer,36 the amputations being partially weight bearing on its end, and the end-bearing stumps being covered with the special skin and pad of the heel, which withstands this weight well. The remainder of the weight is borne through the are of the tibial metaphysis near the top of the prosthesis. This amputation is indicated in trauma, gangrene, and infection and has also been successfully used in patients with congenital limb deformities and deciencies such as bular hemimelia, proximal focal femoral de-
CHAPTER 24
Amputations of the Foot and Ankle
1391
ciency, and congenital pseudarthrosis of the tibia.1,16,22,25 The literature reects that Symes amputation can be done in one or two stages.45 There is little difference except for a slight shift in the position of the initial skin incisions 1.5 cm more distally and anteriorly in the two-stage procedure in order to cover the malleoli, which are not resected in the rst stage. At this time, most authors and surgeons who are experienced in this technique almost exclusively do Symes amputation in one stage. Little evidence exists at this time to demonstrate an advantage or a need for the delayed resection of the malleoli. In the one-stage procedure, the malleoli are cut at the time of the amputation. The malleoli should not be resected in children unless severe pressure problems arise, and then they should be resected below the physeal line. Surgical Technique 1. The anterior incision is along a line that connects two points placed 1 to 1.5 cm below and 1 to 1.5 cm anterior to the midpoint of the tip of each malleolus. The two malleolar points are then connected by an incision
2. 3. 4.
5.
6.
7.
across the sole and perpendicular to its plane (Fig. 2423A and video clip 3). The plantar incision is carried all the way down to bone (i.e., down to the calcaneus). The dorsal incision is carried down to the dome of the talus. The anterior tendons are pulled down with a clamp and divided so that they retract. The anterior tibial artery is ligated or electrocoagulated. The collateral ligament attachments on the talus are divided by alternating back and forth medially to laterally while pulling the talus forward and down (Fig. 2423B). Great care is taken to avoid the neurovascular bundle on the medial side. This is one of the two critical points of the procedure, as was well described by Syme. The bundle lies between the exor hallucis longus and exor digitorum longus tendons and can be accidentally severed. The guide is the exor digitorum longus tendon because the bundle lies just behind it (Fig. 2423B). Once the bone is seen, blunt dissection is used (e.g., with a broad Key elevator) to separate the bone from the entire soft tissue envelope.
A B C
Figure 2423 Technique for Symes amputation. A, Incisions for Symes amputation. The two incisions connect points at 1 cm anterior and 1 cm distal to the tip of each malleolus. B, Incision is carried directly to the bone; subperiosteal dissection of the os calcis is begun. C, Bone hook in the talus for traction. Subperiosteal dissection to the os calcis continues, and the top of the os calcis is dissected. A bone hook in the talus aids in peeling the os calcis out of the soft tissue envelope. D, Skin closure with nylon or other nonabsorbable suture. Note closed incision with dog-ears and a good base of the posterior skin.
1392
PART VI
Diabetes
8. A bone hook in the talus assists in the dissection by applying traction to the interface of bone and soft tissue as the calcaneus is dissected out (Fig. 2423C). 9. This is the second major danger point in the procedure: the subcutaneous attachment of the Achilles tendon. Penetrating or buttonholing through the skin at this point usually dooms the procedure and leads to failure of the Syme stump because of damage to the heel pad. The alternating use of sharp and blunt dissection with scalpel and periosteal elevator works best (Fig. 2423C). This portion of the procedure is responsible for making Symes procedure the most technically difcult foot amputation. 10. The subperiosteal dissection alternates from above at the Achilles tendon and from the undersurface and sides of the calcaneus until the bone is free from the soft tissue. This leaves the hollow of the stump ready for nal shaping and closure. The bundle within the ap is avoided so as not to damage the blood supply to the heel pad. 11. Before performing the closure, the malleoli are cut off ush with the level of the tibial plafond with a saw or with osteotomes. 12. It is not necessary to remove the cartilage from the distal end of the tibia. If the pad appears to be too mobile at closure, additional tissue should be resected from the distal (plantar) edge of the heel pad. 13. Stabilization of the stump can be accomplished using one or several methods. The deep layer of the plantar pad (the plantar fascia included) can be sutured to the anterior edge of the tibia. Alternatively, the plantar fascia can be sutured to the deep fascia over the anterior tibia. Tenodesis of the Achilles tendon has been described.42 14. The closure is done in layers over a suction drain that is brought out proximally through a separate tiny stab wound (Fig. 2423D). 15. The skin is closed with nylon sutures. 16. A bulky, soft dressing is applied, usually followed with a cast. Postoperative Care A cast is usually applied to protect the stump and leg. If the patient is diabetic, nonweight-
bearing ambulation is maintained for 6 weeks. Earlier ambulation in the cast can sometimes be allowed in nondiabetic patients, depending on the progression of wound healing. Although resection of the malleoli to the level of the tibial plafond is required, narrowing the mediallateral are of the tibial metaphysis is contraindicated. The are is required to give a wider base to the bulbous stump. The are is the main structure that holds the prosthesis on and keeps it from slipping up and down. In a two-stage procedure done for infected cases, the second stage is performed about 6 weeks after the initial amputation, provided that satisfactory healing has occurred. At the second stage the dog-ears of soft tissue are reduced medially and laterally and the malleoli are resected through these elliptic incisions (Fig. 2424). Care must be taken not to excessively resect the dog-ears so as not to damage the blood supply to the pad. However, this is not as critical as in a one-stage procedure, because this second stage is not done until the primary suture line is totally healed. The reported success rate of Symes amputations has varied from 50% to 90%.17,26,31,44,45 At this time, most centers report about a 70% success rate for healing of Symes amputations in diabetic and dysvascular patients. The vast majority of failures in this population occur early
Figure 2424 Note medial and lateral dog-ears. The dogears can be excised with an ellipse of skin and soft tissue.
CHAPTER 24
Amputations of the Foot and Ankle
1393
Figure 2426 Ulceration over the distal portion of the bula due to stump mobility 6 years after a Symes amputation. The ulcer healed after resection of the bony prominence.
Figure 2425 Failed Symes amputation due to early gangrene and failure of soft tissue to heal. This was revised to a below-knee amputation.
width of the distal end of the tibia. This tting problem has been handled in several different ways, including placing a hinged window in the prosthesis, placing a wraparound ller above the bulb (Fig. 2427), and using an elastic
as the result of failure to achieve primary wound healing, usually because of vascular insufciency of the heel pad, which is supplied by branches of the posterior tibial artery (Fig. 2425). Late failure of Symes amputation usually results from peripheral vascular disease that progresses to gangrenous changes of the entire lower-limb segment rather than from mechanical complications inherent within the Symes stump. However, some patients can develop pressure lesions over the distal bony prominences that can lead to proximal revision. Mobility of the stump can lead to pressure areas over the distal bula or tibia (Fig. 2426). The treatment is resection of the bula more proximally, or smoothing the tibial edge, and, in a neuropathic patient, debridement or resection of the ulcer as well. As with all neuropathic ulcerations, measures are taken to resect enough bone to relieve pressure and tension on the skin and to debride the soft tissue. An experienced prosthetist must t the prosthesis on the Syme stump. The challenge is that a snug t is required but the wide, bulbous end of the stump must pass through a very narrow portion of the prosthesis corresponding to the
Figure 2427 One type of Symes prosthesis using a wraparound Plastizote sleeve for the narrow part of the leg above the distal bulb.
1394
PART VI
Diabetes
double-wall construction for the distal part of the prosthesis. The best method is the one with which the prosthetist is most familiar and experienced. A disadvantage of Symes amputation compared with a below-knee amputation is that the cosmesis of a Syme stump is reduced because of the wide ankle portion of the prosthesis. In many other ways, the Symes prosthesis is preferable to a below-knee amputation. The Symes stump is partially end bearing and has fewer problems with skin breakdown over the proximal portion of the leg. The mechanical advantage of a full lower-leg segment is enormous and gives great leverage to the quadriceps. Even more important, patients with Symes amputation need minimal prosthetic training compared to patients with a below-knee amputation, because functionally the Symes procedure is a partial foot amputation, and walking in the prosthesis is similar to walking in a cast, which most of the patients have used previously. Symes amputation is functionally superior to proximal procedures such as below-knee and above-knee amputations as demonstrated by studies showing lower energy cost (oxygen consumption per meter) and higher gait velocity and stride length.47 Pitfalls and Complications The most common complication of the Symes procedure in diabetic and dysvascular patients is a failure of healing. Some of these complications cannot be prevented if the goal of sal-
vaging as much of the limb as possible is to be pursued. The second most common problem with this procedure is mobility and displacement of the soft tissue stump. This is addressed through cautious resection of excess soft tissue and by stabilizing the stump. Aggressive resection of the dog-ears on the medial and lateral corners of the stump is a pitfall that results in a dangerously narrowed base to the heel ap. This can reduce the perfusion of the distal pad of the stump and cause the procedure to fail. It is best to leave this excess medial and lateral soft tissue, because it will shrink as the wound heals and the patient assumes use of a prosthesis. In Symes amputations done for trauma, a moderate number of failures are caused by pain of two types. The rst cause is neuroma formation at or above the level of the ankle joint, where the major nerves have been transected. Selective injection is helpful in diagnosis before surgical excision or burying of the neuromas. The second cause is recalcitrant heel pain, seen in patients who have sustained crushing trauma to the heel and hindfoot at the original accident, most of which is industrial in nature. These may need to be revised to a long below-knee amputation. The absolute contraindication to the use of a Symes amputation in any patient is the lack of an intact and viable heel pad. Patients with ulceration or even small gangrenous spots on the heel are not candidates for this procedure and should have a below-knee amputation instead (Fig. 2428A and B).
Figure 2428 This patient has the absolute contraindication for a Symes amputation: soft tissue breakdown over the heel. A, Lateral view. B, Plantar view.
CHAPTER 24
Amputations of the Foot and Ankle
1395
Pirogoffs amputation is a variation on the Syme procedure in which varying amounts of the tubercle of the calcaneus are preserved and then internally xed to the distal cut end of the tibia (Fig. 2429). Longer soft tissue aps are required. The purported advantage of this procedure is its longer length because Symes amputation results in mild shortening, although that can be accommodated in the prosthesis. Pirogoffs procedure obviates the technical difculty of dissecting the Achilles tendon off the calcaneus. However, xation of the calcaneal tubercle to the distal tibia has its own technical difculties, as well as the risk of symptomatic nonunion. It is not widely practiced in the United States at this time.
BELOW-KNEE AMPUTATIONS Below-knee amputations are sometimes the necessary treatment when foot salvage amputations fail. When a below-knee amputation is done for foot disease, consideration should be given to the level of the below-knee resection. The ideal below-knee stump is a minimum of 15 cm (about 6 inches) below the level of the knee joint. Although a slightly longer or shorter stump can be used, variations in length must be taken into consideration in working with the prosthetist in the postoperative manufacture of the below-knee prosthesis. Longer below-knee stumps can afford a longer lever and thus greater power to the musculature about the knee. Longer stumps are favored by me and other authors when a longer stump is appropriate to the tissue healing of an individual patient.40 The amputation stump can be closed with a longer posterior ap or with side-to-side aps. A long posterior ap is easiest and most predictable because it provides excellent distal padding under the resected end of the tibia. Proper shaping of the aps for a posterior ap closure is usually overlooked. Most surgeons learn as interns to cut a square posterior ap. This is easy to remember but leads to a stump with large dog-ears on both sides that ts poorly within a temporary prosthesis. This slows both healing and rehabilitation. If surgical technique is deemed important to the patients outcome in other forms of surgical reconstruction, this should be no exception. The technique for proper shaping of the stump is subtle but simple. Shaping is important because it allows the surgeon to make an amputation stump that is tapered. This allows earlier prosthetic tting because less shrinkage of the stump is necessary. The healing of soft tissue is enhanced as well because the skin edges come together better. The key is to shape the posterior ap to correspond to the cross-sectional shape of the limb. This requires rounding the aps. More importantly, it requires tapering the ap by making the midportion of the ap widest to correspond to the diameter of the leg and making the distal part of the ap narrow to correspond to the anterior width of the limb (Fig. 2430).
Lines of bone resection
Os calcis Pirogoffs amputation
Figure 2429
Technique for Pirogoffs amputation.
1396
PART VI
Diabetes
Skin incisions for a tapered BKA stump
AI BI LEG Level and shape of tibial resection B FLAP A
Figure 2430 A long below-knee amputation (BKA) has mechanical advantages and is often possible when done for foot disease that does not extend above the ankle. Lines A and A and B and B are, respectively, the matching widths of the leg and of the posterior ap that produce a tapered BKA stump. A square posterior ap always produces dog-ears, which slow the shaping of the BKA stump for tting the rst prosthesis.
SUMMARY
Although amputation of the foot is an unfortunate necessity for some patients, attention to detail, both in diagnostic evaluation and in surgical technique, improves the surgeons ability to assist patients successfully in this major step toward rehabilitation of function and ambulation. All photographs in this chapter are copyrighted by James W. Brodsky, MD. REFERENCES
1. Anderson L, Westin GW, Oppenheim WL: Syme amputation in children: Indications, results, and long-term follow-up. J Pediatr Orthop 4:550-554, 1984.
2. Anderson RB, Foster MD, Gould JS, et al: Free tissue transfer and calcanectomy as treatment of chronic osteomyelitis of the os calcis: A case report. Foot Ankle 11:168-171, 1990. 3. Apelqvist J, Castenfors J, J L, et al: Prognostic value of systolic ankle and of blood pressure levels in outcome of diabetic foot ulcer. Diabetes Care 12:373-378, 1989. 4. Armstrong DG, Hadi S, Nguyen HC, et al: Factors associated with bone regrowth following diabetes-related partial amputation of the foot. J Bone Joint Surg Am 81:1561-1565, 1999. 5. Biehl WC 3rd, Morgan JM, Wagner FW Jr, et al: The safety of the Esmarch tourniquet. Foot Ankle 14:278-283, 1993. 6. Brodsky JW: Amputations of the foot and ankle. In Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St. Louis, Mosby, 1993. 7. Burgess EM, Marsden FW: Major lower extremity amputations following arterial reconstruction. Arch Surg 108:655-660, 1974. 8. Chang BB, Bock DE, Jacobs RL, et al: Increased limb salvage by the use of unconventional foot amputations. J Vasc Surg 19:341348; discussion 348-349, 1994.
CHAPTER 24
Amputations of the Foot and Ankle
1397
9. Christie J, Clowes CB, Lamb DW: Amputations through the middle part of the foot. J Bone Joint Surg Br 62:473-474, 1980. 10. Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 23:896-901, 2002. 11. Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St. Louis, Mosby, 1999. 12. Crandall RC, Wagner FW, Jr.: Partial and total calcanectomy: A review of thirty-one consecutive cases over a ten-year period. J Bone Joint Surg Am 63:152-155, 1981. 13. Dickhaut SC, DeLee JC, Page CP: Nutritional status: Importance in predicting wound-healing after amputation. J Bone Joint Surg Am 66:71-75, 1984. 14. Due TM, Jacobs RL: Molded foot orthosis after great toe or medial ray amputations in diabetic feet. Foot Ankle 6:150-152, 1985. 15. Eginton MT, Brown KR, Seabrook GR, et al: A prospective randomized evaluation of negative-pressure wound dressings for diabetic foot wounds. Ann Vasc Surg 17:645-649, 2003. 16. Fergusson CM, Morrison JD, Kenwright J: Leg-length inequality in children treated by Symes amputation. J Bone Joint Surg Br 69:433-436, 1987. 17. Francis H 3rd, Roberts JR, Clagett GP, et al: The Syme amputation: Success in elderly diabetic patients with palpable ankle pulses. J Vasc Surg 12:237-240, 1990. 18. Giacalone VF, Gregory JL, Krych SM: Calcanectomy for the treatment of calcaneal osteomyelitis. A case report. J Am Podiatr Med Assoc 81:88-92, 1991. 19. Goldner MG: The fate of the second leg in the diabetic amputee. Diabetes 9:100-103, 1960. 20. Harris RI: Symes amputation; the technical details essential for success. J Bone Joint Surg Br 38:614-632, 1956. 21. Harris WR, Silverstein EA: Partial amputations of the foot: A follow-up study. Can J Surg 41:6-11, 1964. 22. Herring JA, Barnhill B, Gaffney C: Syme amputation. An evaluation of the physical and psychological function in young patients. J Bone Joint Surg Am 68:573-578, 1986. 23. Hodge MJ, Peters TG, Erd WG: Amputation of the distal portion of the foot. South Med J 82:1138-1142, 1989. 24. Isenberg JS, Costigan WM, Thordarson DB: Subtotal calcanectomy for osteomyelitis of the os calcis: A reasonable alternative to free tissue transfer. Ann Plast Surg 35:660-663, 1995. 25. Jacobsen ST, Crawford AH, Millar EA, et al: The Syme amputation in patients with congenital pseudarthrosis of the tibia. J Bone Joint Surg Am 65:533-537, 1983. 26. Jany RS, Burkus JK: Long-term follow-up of Syme amputations for peripheral vascular disease associated with diabetes mellitus. Foot Ankle 9:107-110, 1988. 27. Larsson U, Andersson GB: Partial amputation of the foot for diabetic or arteriosclerotic gangrene. Results and factors of prognostic value. J Bone Joint Surg Br 60:126-130, 1978. 28. Lieberman JR, Jacobs RL, Goldstock L, et al: Chopart amputation with percutaneous heel cord lengthening. Clin Orthop Relat Res 296:86-91, 1993. 29. Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St. Louis, Mosby, 1993. 30. McCallon SK, Knight CA, Valiulus JP, et al: Vacuum-assisted closure versus saline-moistened gauze in the healing of post-
31. 32.
33.
34.
35.
36. 37.
38.
39.
40. 41.
42.
43.
44. 45.
46. 47.
48.
49. 50.
operative diabetic foot wounds. Ostomy Wound Manage 46:2832, 34, 2000. McElwain JP, Hunter GA, English E: Symes amputation in adults: A long-term review. Can J Surg 28:203-205, 1985. McKittrick LS, McKittrick JB, Risley TS: Transmetatarsal amputation for infection or gangrene in patients with diabetes mellitus. J Am Podiatr Med Assoc 83:62-78, 1949. Millstein SG, McCowan SA, Hunter GA: Traumatic partial foot amputations in adults. A long-term review. J Bone Joint Surg Br 70:251-254, 1988. Moore WS: Determination of amputation level. Measurement of skin blood ow with xenon Xe 133. Arch Surg 107:798-802, 1973. Mueller MJ, Sinacore DR, Hastings MK, et al: Effect of Achilles tendon lengthening on neuropathic plantar ulcers. A randomized clinical trial. J Bone Joint Surg Am 85:1436-1445, 2003. Nakhgevany KB, Rhoads JE, Jr.: Ankle-level amputation. Surgery 95:549-552, 1984. Oishi CS, Fronek A, Golbranson FL: The role of non-invasive vascular studies in determining levels of amputation. J Bone Joint Surg Am 70:1520-1530, 1988. Roach JJ, Deutsch A, McFarlane DS: Resurrection of the amputations of Lisfranc and Chopart for diabetic gangrene. Arch Surg 122:931-934, 1987. Saltzman CL: Salvage of diffuse ankle osteomyelitis by singlestage resection and circumferential frame compression arthrodesis. Iowa Orthop J 25:47-52, 2005. Smith DG: Principles of partial foot amputations in the diabetic. Instr Course Lect 48:321-329, 1999. Smith DG, Boyko EJ, Ahroni JH, et al: Paradoxical transcutaneous oxygen response to cutaneous warming on the plantar foot surface: A caution for interpretation of plantar foot TcPO2 measurements. Foot Ankle Int 16:787-791, 1995. Smith DG, Sangeorzan BJ, Hansen ST Jr, et al: Achilles tendon tenodesis to prevent heel pad migration in the Symes amputation. Foot Ankle Int 15:14-17, 1994. Smith DG, Stuck RM, Ketner L, et al: Partial calcanectomy for the treatment of large ulcerations of the heel and calcaneal osteomyelitis. An amputation of the back of the foot. J Bone Joint Surg Am 74:571-576, 1992. Spittler AW, Brennan JJ, Payne JW: Syme amputation performed in two stages. J Bone Joint Surg Am 36:37-42; passim, 1954. Wagner F: The diabetic foot and amputations of the foot. In Mann R (ed): Surgery of the Foot. St. Louis, MosbyYear Book, 1986. Wagner FW, Jr: Amputations of the foot and ankle. Current status. Clin Orthop Relat Res Jan-Feb(122):62-69, 1977. Waters RL, Perry J, Antonelli D, et al: Energy cost of walking of amputees: The inuence of level of amputation. J Bone Joint Surg Am 58:42-46, 1976. Weisenfeld LS, Flannery D, Luzzi A, et al: Partial calcanectomy for the treatment of osteomyelitis of the os calcis. J Foot Surg 29:226-230, 1990. Woll TS, Beals RK: Partial calcanectomy for the treatment of osteomyelitis of the calcaneus. Foot Ankle 12:31-34, 1991. Wyss CR, Harrington RM, Burgess EM, et al: Transcutaneous oxygen tension as a predictor of success after an amputation. J Bone Joint Surg Am 70:203-207, 1988.
También podría gustarte
- Fungal Nail and Ingrown Toenail GuideDocumento60 páginasFungal Nail and Ingrown Toenail GuideAmar AlkhafajiAún no hay calificaciones
- Ankle Arthrodesis - Screw FixationDocumento26 páginasAnkle Arthrodesis - Screw FixationChristopher HoodAún no hay calificaciones
- Laor FootDocumento77 páginasLaor FootTrandafir LacramioaraAún no hay calificaciones
- Sample Chapter Coughlin Mann's Surgery of The Foot and Ankle 9780323072427 PDFDocumento34 páginasSample Chapter Coughlin Mann's Surgery of The Foot and Ankle 9780323072427 PDFodi jayaAún no hay calificaciones
- The Foot and Ankle in Rheumatoid ArtritisDocumento229 páginasThe Foot and Ankle in Rheumatoid ArtritislanuzalteaAún no hay calificaciones
- Relieve Pain and Improve Mobility With Knee ImplantsDocumento6 páginasRelieve Pain and Improve Mobility With Knee ImplantsMoses DhinakarAún no hay calificaciones
- Review - Presby Residency ManualDocumento400 páginasReview - Presby Residency ManualSneha SutharAún no hay calificaciones
- Chapter 3e Pathological GaitDocumento8 páginasChapter 3e Pathological GaitpodmmgfAún no hay calificaciones
- Chapter 5 Pediatric PodiatryDocumento88 páginasChapter 5 Pediatric Podiatrypodmmgf100% (1)
- Foot and Ankle Anatomy and Physical Examination PART 1Documento49 páginasFoot and Ankle Anatomy and Physical Examination PART 1eric sivaneshAún no hay calificaciones
- ABFAS Study GuideDocumento368 páginasABFAS Study GuideMohammed FarhanAún no hay calificaciones
- OITE ReviewDocumento154 páginasOITE ReviewPanagiotis Poulios100% (2)
- Clubfoot Guide: Causes, Symptoms & TreatmentDocumento17 páginasClubfoot Guide: Causes, Symptoms & TreatmentMulya ImansyahAún no hay calificaciones
- Handbook of Foot and Ankle Orthopedics (Rational Prescription of Foot and Ankle Orthotics) PDFDocumento6 páginasHandbook of Foot and Ankle Orthopedics (Rational Prescription of Foot and Ankle Orthotics) PDFAbdallah Jaber100% (2)
- Actures of The Midfoot and ForefootDocumento37 páginasActures of The Midfoot and ForefootMrHadezz LamerAún no hay calificaciones
- Modified Direct Lateral Approach for Total Hip ArthroplastyDocumento5 páginasModified Direct Lateral Approach for Total Hip ArthroplastyscribdfoaktAún no hay calificaciones
- AAOS2007 Pediatric PDFDocumento58 páginasAAOS2007 Pediatric PDFHéctor Pando SánchezAún no hay calificaciones
- Post-Op Rehab of Tibia/Fibula ORIFDocumento75 páginasPost-Op Rehab of Tibia/Fibula ORIFExternalAún no hay calificaciones
- Alingment in TKRDocumento3 páginasAlingment in TKRdeepak100% (1)
- @MedicalBooksStore 2013 ExternalDocumento431 páginas@MedicalBooksStore 2013 ExternalОлександр ШендераAún no hay calificaciones
- Lower Extremity DisordersDocumento25 páginasLower Extremity DisordersJameson87Aún no hay calificaciones
- Management of Patellofemoral Chondral InjuriesDocumento24 páginasManagement of Patellofemoral Chondral InjuriesBenalAún no hay calificaciones
- Ankle Stability and MovementDocumento40 páginasAnkle Stability and MovementBogdan GeangosAún no hay calificaciones
- Pediatric Knee Injuries: Greg M. Osgood, MDDocumento101 páginasPediatric Knee Injuries: Greg M. Osgood, MDkosmynin86100% (1)
- Charnley Ankle ArthrodesisDocumento12 páginasCharnley Ankle Arthrodesisdr_s_ganeshAún no hay calificaciones
- Tennis Elbow JOSPT ArticleDocumento11 páginasTennis Elbow JOSPT ArticleHasan RahmanAún no hay calificaciones
- Calcaneus Fracture: Randy SusantoDocumento32 páginasCalcaneus Fracture: Randy SusantoRandy SusantoAún no hay calificaciones
- Distal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiDocumento5 páginasDistal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiPhysiotherapy Care SpecialistsAún no hay calificaciones
- New Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauDocumento8 páginasNew Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauCosmina BribanAún no hay calificaciones
- TFCCDocumento22 páginasTFCChmtno3100% (1)
- @ankle BreakerDocumento2 páginas@ankle BreakerEGAún no hay calificaciones
- Krozer ManualDocumento148 páginasKrozer Manualpoddata100% (3)
- External Fixation Indications and Techniques (BONATUS)Documento47 páginasExternal Fixation Indications and Techniques (BONATUS)Ayi Zulher0% (1)
- Queens Orthopedic Inpatient Trauma PDFDocumento27 páginasQueens Orthopedic Inpatient Trauma PDFRema AmerAún no hay calificaciones
- 2007 JBJS External Fixation How To Make It Work PDFDocumento15 páginas2007 JBJS External Fixation How To Make It Work PDFsuad5stambulieAún no hay calificaciones
- Locked Plating: Sean E. Nork, MD James P. Stannard, MD and Philip J. Kregor, MDDocumento119 páginasLocked Plating: Sean E. Nork, MD James P. Stannard, MD and Philip J. Kregor, MDDeep Katyan DeepAún no hay calificaciones
- AAOS2012 Foot and AnkleDocumento103 páginasAAOS2012 Foot and AnkleAmmar HilliAún no hay calificaciones
- Dance Injuries-Foot and AnkleDocumento7 páginasDance Injuries-Foot and Ankleapi-198787605100% (1)
- Congenital Clubfoot TreatmentDocumento23 páginasCongenital Clubfoot TreatmentBernard Santoso0% (2)
- AAOS Mini Open Rotator Cuff RepairDocumento10 páginasAAOS Mini Open Rotator Cuff RepairHannah CoAún no hay calificaciones
- Chemical Hip Denervation For Inoperable Hip FractureDocumento6 páginasChemical Hip Denervation For Inoperable Hip Fracturemanuel torresAún no hay calificaciones
- Oh My Painful FOOT!!!: Plantar FasciitisDocumento20 páginasOh My Painful FOOT!!!: Plantar FasciitisAsogaa MeteranAún no hay calificaciones
- Hanger PDRDocumento63 páginasHanger PDRTetay JavierAún no hay calificaciones
- Approach To FractureDocumento17 páginasApproach To FractureRebecca WongAún no hay calificaciones
- The Foot and AnkleDocumento17 páginasThe Foot and Ankletimmaber100% (1)
- Infection in Orthopedic SurgeryDocumento17 páginasInfection in Orthopedic SurgerykesramanujamAún no hay calificaciones
- Arthrodesis Techniques in The Management of Stage II and III Acquired Adult Flatfoot Deformity.Documento12 páginasArthrodesis Techniques in The Management of Stage II and III Acquired Adult Flatfoot Deformity.C Martin TraumatoAún no hay calificaciones
- Inramedullarynailingpptfinal 160902185707Documento65 páginasInramedullarynailingpptfinal 160902185707Pankaj VatsaAún no hay calificaciones
- 2004, Vol.23, Issues 1, Athletic Foot and Ankle InjuriesDocumento165 páginas2004, Vol.23, Issues 1, Athletic Foot and Ankle InjuriesAndrei Gianina100% (3)
- Ortho Instruments & ImplantsDocumento106 páginasOrtho Instruments & ImplantsBi PinAún no hay calificaciones
- Handbook of Foot and Ankle Orthopedics (Foot&AnkleExamination) PDFDocumento22 páginasHandbook of Foot and Ankle Orthopedics (Foot&AnkleExamination) PDFAbdallah JaberAún no hay calificaciones
- Synthes Titanium Implant PlatesDocumento36 páginasSynthes Titanium Implant PlatesMico StanojevicAún no hay calificaciones
- Pain Scale For Plantar FasciiitsDocumento6 páginasPain Scale For Plantar FasciiitsAnna HipAún no hay calificaciones
- Orthotics Consensus Conference ReportDocumento354 páginasOrthotics Consensus Conference ReportAlec joshua RapadaAún no hay calificaciones
- Hershey Board Certification Review Outline Study Guide: Jonathan M. Singer, D.P.MDocumento9 páginasHershey Board Certification Review Outline Study Guide: Jonathan M. Singer, D.P.MpoddataAún no hay calificaciones
- Wrist Anatomy: Bones Quiz - What Bones Comprise The Wrist? Joints Quiz - What Joints Comprise The Wrist?Documento63 páginasWrist Anatomy: Bones Quiz - What Bones Comprise The Wrist? Joints Quiz - What Joints Comprise The Wrist?Mnn SaabAún no hay calificaciones
- Orthopaedic Management in Cerebral Palsy, 2nd EditionDe EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannCalificación: 3 de 5 estrellas3/5 (2)
- Microsurgical Skills: A Handbook of Experimental Microsurgical TechniquesDe EverandMicrosurgical Skills: A Handbook of Experimental Microsurgical TechniquesAún no hay calificaciones
- Pe Hope 11 PDFDocumento81 páginasPe Hope 11 PDFRezaej BiliranAún no hay calificaciones
- ExercíciosDocumento2 páginasExercíciosvatomarnocuAún no hay calificaciones
- Cartridge Filter Pump RX600-1500Documento24 páginasCartridge Filter Pump RX600-1500Juliano PereiraAún no hay calificaciones
- Doane Pain PDFDocumento65 páginasDoane Pain PDFOmar Ba100% (1)
- Neurological AssessmentDocumento12 páginasNeurological AssessmentMushtaha Ibrahim100% (1)
- Beginner's Guide to Barbell TrainingDocumento20 páginasBeginner's Guide to Barbell TrainingDamjan Josovic100% (1)
- P.E-1 Module 6Documento10 páginasP.E-1 Module 6Sean Michael ComprendioAún no hay calificaciones
- Progressive Muscle Relaxation Script: Adapted From The Anxiety & Phobia Workbook, by Edmund J. BourneDocumento3 páginasProgressive Muscle Relaxation Script: Adapted From The Anxiety & Phobia Workbook, by Edmund J. BourneAkash LuhanaAún no hay calificaciones
- AD&D Adventure Gamebooks Lords of DoomDocumento195 páginasAD&D Adventure Gamebooks Lords of DoomWerewolf67100% (4)
- Mckenzie Vs William Flexion ExerciseDocumento38 páginasMckenzie Vs William Flexion ExerciseIftinan AmaliaAún no hay calificaciones
- Understanding Normal & Pathological GaitDocumento44 páginasUnderstanding Normal & Pathological GaitJean Pascal AppadooAún no hay calificaciones
- PARTOGRAPHDocumento49 páginasPARTOGRAPHMhianne SarmientoAún no hay calificaciones
- ANAT1012.1019 Example Regional Lower Limb SAQ's - 2022Documento3 páginasANAT1012.1019 Example Regional Lower Limb SAQ's - 2022Grace YAún no hay calificaciones
- Name: Josiah Guenn P. Villaraza Group: B Clinical Instructor: Ma'am Irene Cheeries Apal-Enriquez, RN Date: November 7, 2021Documento3 páginasName: Josiah Guenn P. Villaraza Group: B Clinical Instructor: Ma'am Irene Cheeries Apal-Enriquez, RN Date: November 7, 2021Princess EduaveAún no hay calificaciones
- Home Economics Beauty/Nail Care Services Quarter 1 - Module 1 Apply Hand TreatmentDocumento15 páginasHome Economics Beauty/Nail Care Services Quarter 1 - Module 1 Apply Hand Treatmentmarygrace cano100% (2)
- The Effect of Arch Height and Material Hardness ofDocumento9 páginasThe Effect of Arch Height and Material Hardness ofalexAún no hay calificaciones
- Post Natal Exercise PlanDocumento18 páginasPost Natal Exercise PlanSathya BharathiAún no hay calificaciones
- Excavation Safety ChecklistDocumento2 páginasExcavation Safety Checklistsindarth raveendrakrishnanAún no hay calificaciones
- Ankle exercises for rehabilitationDocumento3 páginasAnkle exercises for rehabilitationJohn NixonAún no hay calificaciones
- Russell's Guide to Bird Feet and NestsDocumento2 páginasRussell's Guide to Bird Feet and NestsCassie WoolleyAún no hay calificaciones
- Full Script Teaching Physical Education Weak 11 - Assa Saesar NurdiansyahDocumento4 páginasFull Script Teaching Physical Education Weak 11 - Assa Saesar NurdiansyahAssa Saesar NurdiansyahAún no hay calificaciones
- Start Here Horizontal Pull Vertical Push Core Vertical Pull Handstand Horizontal Push Warm-UpDocumento31 páginasStart Here Horizontal Pull Vertical Push Core Vertical Pull Handstand Horizontal Push Warm-UpRazvan MihaiAún no hay calificaciones
- Httpskundaliniyogawageningen - NLWP Contentuploads201805Seventh Body Meditation and Excercises PDFDocumento5 páginasHttpskundaliniyogawageningen - NLWP Contentuploads201805Seventh Body Meditation and Excercises PDFMarleen van LokvenAún no hay calificaciones
- Full Body Workout 30 MinuteDocumento8 páginasFull Body Workout 30 MinuteFelicia Angelini TaroreAún no hay calificaciones
- WB-2736 Flammable Combustible Storage Room PDFDocumento2 páginasWB-2736 Flammable Combustible Storage Room PDFRain KongAún no hay calificaciones
- Ana Cheri - H.I.I.T Your Target PDFDocumento51 páginasAna Cheri - H.I.I.T Your Target PDFKostyaAún no hay calificaciones
- UNIT I Movement EnhancementDocumento7 páginasUNIT I Movement EnhancementKervin Rey Guevarra JacksonAún no hay calificaciones
- Wcms 650136Documento30 páginasWcms 650136Goran SpasićAún no hay calificaciones
- The Accessory Navicular and Its Pertinence To DancersDocumento12 páginasThe Accessory Navicular and Its Pertinence To Dancerscalley2Aún no hay calificaciones
- Self-Learning H Ome Task (SLHT)Documento11 páginasSelf-Learning H Ome Task (SLHT)Angela Gabrielle O BagadiongAún no hay calificaciones