También podría gustarte
- Price Transmission Notions and Components and TheDocumento4 páginasPrice Transmission Notions and Components and TheYaronBabaAún no hay calificaciones
- Jack Johnston, John DiNardo Econometric Methods, Fourth Edition PDFDocumento514 páginasJack Johnston, John DiNardo Econometric Methods, Fourth Edition PDFMarcelo Rodrigo Riffo67% (3)
- Food Security Status in NigeriaDocumento16 páginasFood Security Status in NigeriaYaronBabaAún no hay calificaciones
- Local Engagement Liaison OfficerDocumento2 páginasLocal Engagement Liaison OfficerYaronBabaAún no hay calificaciones
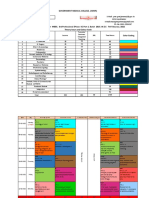
- No. Variables Pbefore Pafter Wbefore Wafter BwithDocumento2 páginasNo. Variables Pbefore Pafter Wbefore Wafter BwithYaronBabaAún no hay calificaciones
- Price Transmission Notions and Components and TheDocumento4 páginasPrice Transmission Notions and Components and TheYaronBabaAún no hay calificaciones
- A Price Transmission Testing FrameworkDocumento4 páginasA Price Transmission Testing FrameworkYaronBabaAún no hay calificaciones
- Tranform Roat EdDocumento4 páginasTranform Roat EdYaronBabaAún no hay calificaciones
- Top Social Media Platforms by Component MatrixDocumento1 páginaTop Social Media Platforms by Component MatrixYaronBabaAún no hay calificaciones
- Opening Bank Account by The Vulnerable GroupsDocumento4 páginasOpening Bank Account by The Vulnerable GroupsYaronBabaAún no hay calificaciones
- SR - No. Investmentinputs Noimpact (0) P Littleimpact (1) P Greatimpact (2) P Totalproduct (P) %Documento1 páginaSR - No. Investmentinputs Noimpact (0) P Littleimpact (1) P Greatimpact (2) P Totalproduct (P) %YaronBabaAún no hay calificaciones
- Micro Credit Impact On InvestmentsDocumento2 páginasMicro Credit Impact On InvestmentsYaronBabaAún no hay calificaciones
- Multiple Regression Analyses of The Investments' InputsDocumento4 páginasMultiple Regression Analyses of The Investments' InputsYaronBabaAún no hay calificaciones
- Savings Capacity of The Vulnerable GroupsDocumento4 páginasSavings Capacity of The Vulnerable GroupsYaronBabaAún no hay calificaciones
- Out-Reach and Impact of TheDocumento5 páginasOut-Reach and Impact of TheYaronBabaAún no hay calificaciones
- Impact of Investments Inputs On Productivity AnalysisDocumento2 páginasImpact of Investments Inputs On Productivity AnalysisYaronBabaAún no hay calificaciones
- Changes in Agricultural Investment With Micro CreditDocumento4 páginasChanges in Agricultural Investment With Micro CreditYaronBabaAún no hay calificaciones
- Adp 2013Documento19 páginasAdp 2013YaronBabaAún no hay calificaciones
- Investments Capacity Pattern With Micro CreditDocumento2 páginasInvestments Capacity Pattern With Micro CreditYaronBabaAún no hay calificaciones
- Analyses of Changes in Agricultural Investment With Micro CreditDocumento4 páginasAnalyses of Changes in Agricultural Investment With Micro CreditYaronBabaAún no hay calificaciones
- Opening Bank Account by The Vulnerable GroupsDocumento4 páginasOpening Bank Account by The Vulnerable GroupsYaronBabaAún no hay calificaciones
- Accounting For Wealth in The Measurement of Household IncomeDocumento24 páginasAccounting For Wealth in The Measurement of Household IncomeYaronBabaAún no hay calificaciones
- Analyzing impacts and outreach of microcredit in Borno StateDocumento3 páginasAnalyzing impacts and outreach of microcredit in Borno StateYaronBabaAún no hay calificaciones
- Analysis of Investments Capacity Pattern With Micro CreditDocumento2 páginasAnalysis of Investments Capacity Pattern With Micro CreditYaronBabaAún no hay calificaciones
- Frontier Functions: Stochastic Frontier Analysis (SFA) & Data Envelopment Analysis (DEA)Documento45 páginasFrontier Functions: Stochastic Frontier Analysis (SFA) & Data Envelopment Analysis (DEA)YaronBaba100% (1)
- Accounting For Wealth in The Measurement of Household IncomeDocumento24 páginasAccounting For Wealth in The Measurement of Household IncomeYaronBabaAún no hay calificaciones
- Analyses of Changes in Agricultural Investment With Micro CreditDocumento4 páginasAnalyses of Changes in Agricultural Investment With Micro CreditYaronBabaAún no hay calificaciones
- Table Template For State Report2013Documento19 páginasTable Template For State Report2013YaronBabaAún no hay calificaciones
- Understanding Econometric Analysis UsingDocumento13 páginasUnderstanding Econometric Analysis UsingYaronBabaAún no hay calificaciones
- Tables For 2013 Zonal ReportDocumento22 páginasTables For 2013 Zonal ReportYaronBabaAún no hay calificaciones
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- UtangDocumento11 páginasUtangmaimaiAún no hay calificaciones
- Role of IgraDocumento8 páginasRole of IgraLinda MaylianaAún no hay calificaciones
- Chapter 1Documento7 páginasChapter 1Jeremias Cruz CalaunanAún no hay calificaciones
- Anti-Tb DrugsDocumento26 páginasAnti-Tb DrugsRavi ChandraAún no hay calificaciones
- Determinants of HealthDocumento29 páginasDeterminants of HealthMayom Mabuong92% (12)
- Pamplet - English PDFDocumento4 páginasPamplet - English PDF9884288233100% (1)
- PresentasiDocumento30 páginasPresentasiagusAún no hay calificaciones
- NCLEX Questions PulmDocumento27 páginasNCLEX Questions PulmAnthony Hawley100% (2)
- Anthropology and The Changing World How Can AnthroDocumento12 páginasAnthropology and The Changing World How Can AnthrorahulmalikbrandAún no hay calificaciones
- Group-6 ReviewerDocumento24 páginasGroup-6 ReviewerMaryjel Carlom SumambotAún no hay calificaciones
- TB & MDR TB Guideline 2021Documento249 páginasTB & MDR TB Guideline 2021ali100% (1)
- Form Thông Tin Xin VisaDocumento11 páginasForm Thông Tin Xin VisaNguyễn Tâm AnhAún no hay calificaciones
- Environmental Hazards For The Nurse As A Worker - Nursing Health, & Environment - NCBI Bookshelf PDFDocumento6 páginasEnvironmental Hazards For The Nurse As A Worker - Nursing Health, & Environment - NCBI Bookshelf PDFAgung Wicaksana100% (1)
- The Immune Response in Tuberculosis: FurtherDocumento55 páginasThe Immune Response in Tuberculosis: Furtheranon_430470001Aún no hay calificaciones
- Recent TB Treatment GuidelinesDocumento28 páginasRecent TB Treatment GuidelinesDr venkatesh jalluAún no hay calificaciones
- References Stigma and EpidemicsDocumento280 páginasReferences Stigma and EpidemicsadripfAún no hay calificaciones
- Identification and Classification According To Bergy's Manual of Systemic Bacteriology 2Documento46 páginasIdentification and Classification According To Bergy's Manual of Systemic Bacteriology 2Cezar Alexander GuevaraAún no hay calificaciones
- 609-Article Text-1082-2-10-20190708Documento10 páginas609-Article Text-1082-2-10-20190708Nova RizkenAún no hay calificaciones
- Letterhead Hospital MiriDocumento9 páginasLetterhead Hospital MiriShahir HassanAún no hay calificaciones
- Tuberculosis UNIVALLEDocumento33 páginasTuberculosis UNIVALLEPaz VidaAún no hay calificaciones
- Micro Buzz Words - KEY WordsDocumento8 páginasMicro Buzz Words - KEY WordsKris GulleyAún no hay calificaciones
- Problems On EpidemiologyDocumento146 páginasProblems On EpidemiologyAnnie HadassahAún no hay calificaciones
- Lindsey Bradforf Pioneers of Homeopathy PDFDocumento655 páginasLindsey Bradforf Pioneers of Homeopathy PDFBikash AhmedAún no hay calificaciones
- Lecture 1 - Smear Positive PTBDocumento40 páginasLecture 1 - Smear Positive PTBNasibah Tuan YaacobAún no hay calificaciones
- Audit Kematian Pesakit Tibi 2015Documento72 páginasAudit Kematian Pesakit Tibi 2015Muhammad KhairiAún no hay calificaciones
- Unit 3 Quantificatin Technique For Medicne ProcDocumento2 páginasUnit 3 Quantificatin Technique For Medicne ProcRajan Manandhar ShambhavAún no hay calificaciones
- 18 B Phase III MBBS Part I Teaching Schedule (Theory)Documento40 páginas18 B Phase III MBBS Part I Teaching Schedule (Theory)راجا حسیب میرAún no hay calificaciones
- CHN HandiesDocumento23 páginasCHN HandiesFreeNursingNotesAún no hay calificaciones
- General Principles of Microbial Pathogenesis: MicrobiologyDocumento5 páginasGeneral Principles of Microbial Pathogenesis: MicrobiologyAbi SulitAún no hay calificaciones
- Case Presentation On: TB Meningitis and Hepatitis B, HTNDocumento26 páginasCase Presentation On: TB Meningitis and Hepatitis B, HTNAntoAún no hay calificaciones