También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (894)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (73)
- Medication Competency Questions For NursesDocumento13 páginasMedication Competency Questions For NursesAlex AndrewAún no hay calificaciones
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- Incidence and Factors Related To Flare-Ups in A Graduate Endodontic ProgrammeDocumento7 páginasIncidence and Factors Related To Flare-Ups in A Graduate Endodontic ProgrammeRose FlawerAún no hay calificaciones
- Parthasarathy2013 PDFDocumento7 páginasParthasarathy2013 PDFAndi BintangAún no hay calificaciones
- 1 s2.0 S0002937803001388 MainDocumento3 páginas1 s2.0 S0002937803001388 MainAndi BintangAún no hay calificaciones
- Medical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TDocumento3 páginasMedical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TAndi BintangAún no hay calificaciones
- Subarachnoid Block For Caesarean Section in Severe PreeclampsiaDocumento6 páginasSubarachnoid Block For Caesarean Section in Severe PreeclampsiaAndi BintangAún no hay calificaciones
- 1 s2.0 S0002937803001388 MainDocumento3 páginas1 s2.0 S0002937803001388 MainAndi BintangAún no hay calificaciones
- Depresión e InmunidadDocumento13 páginasDepresión e InmunidadgabisaenaAún no hay calificaciones
- Bar A Zanchi 2018Documento17 páginasBar A Zanchi 2018Andi BintangAún no hay calificaciones
- Anestesia General para Césarea PDFDocumento7 páginasAnestesia General para Césarea PDFAgnese ValentiniAún no hay calificaciones
- Anestesia General para Césarea PDFDocumento7 páginasAnestesia General para Césarea PDFAgnese ValentiniAún no hay calificaciones
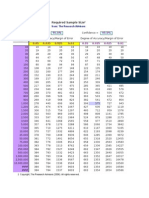
- Required Sample Size: From: The Research AdvisorsDocumento3 páginasRequired Sample Size: From: The Research AdvisorsAbhishek Sharma100% (1)
- Procalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaDocumento5 páginasProcalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaAndi BintangAún no hay calificaciones
- 1 s2.0 S0002937800704534 Main PDFDocumento1 página1 s2.0 S0002937800704534 Main PDFAndi BintangAún no hay calificaciones
- Cultural Sociology of Mental Illness n28Documento5 páginasCultural Sociology of Mental Illness n28Andi BintangAún no hay calificaciones
- Overweight linked to increased risk of lower back painDocumento8 páginasOverweight linked to increased risk of lower back painAndi BintangAún no hay calificaciones
- Instruction For Author ClimactericDocumento9 páginasInstruction For Author ClimactericAndi BintangAún no hay calificaciones
- 1 s2.0 S1052305714000561 MainDocumento6 páginas1 s2.0 S1052305714000561 MainAndi BintangAún no hay calificaciones
- Hepatitis C APASLfghDocumento27 páginasHepatitis C APASLfghAndi BintangAún no hay calificaciones
- Sacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityDocumento5 páginasSacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityAndi BintangAún no hay calificaciones
- 1 s2.0 S0021755713002003 MainDocumento6 páginas1 s2.0 S0021755713002003 MainAndi BintangAún no hay calificaciones
- 1 s2.0 S0021755713002003 MainDocumento6 páginas1 s2.0 S0021755713002003 MainAndi BintangAún no hay calificaciones
- Association Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesDocumento10 páginasAssociation Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesAndi BintangAún no hay calificaciones
- 2013 Student Membership ApplicationDocumento1 página2013 Student Membership ApplicationAndi BintangAún no hay calificaciones
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationDocumento6 páginasPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangAún no hay calificaciones
- Anthropometry: Ergonomics Additional ResourcesDocumento5 páginasAnthropometry: Ergonomics Additional ResourcesAndi BintangAún no hay calificaciones
- Serviks DocjhjuDocumento366 páginasServiks DocjhjuAndi BintangAún no hay calificaciones
- Urologi PDFDocumento237 páginasUrologi PDFAndi BintangAún no hay calificaciones
- MK Giz Slide Infant Feeding PracticeDocumento1 páginaMK Giz Slide Infant Feeding PracticeAndi BintangAún no hay calificaciones
- ATS Guidelines CAP ManagementDocumento25 páginasATS Guidelines CAP ManagementMae Matira AbeladorAún no hay calificaciones
- PCT CAP ABiuytoDocumento10 páginasPCT CAP ABiuytoAndi BintangAún no hay calificaciones
- Cap Bts 2009 ComplitdgDocumento139 páginasCap Bts 2009 ComplitdgAndi BintangAún no hay calificaciones
- IJMRHS VOl 3 Issue 3 With Cover Page v2Documento272 páginasIJMRHS VOl 3 Issue 3 With Cover Page v2Muhammad ZubairAún no hay calificaciones
- Model Question Papers AnmDocumento8 páginasModel Question Papers AnmAbhijit Sanjeev77% (13)
- DiabetesDocumento515 páginasDiabetesPaola Rivera DiazAún no hay calificaciones
- 7 Case Definitions of Infectious Disease in MalaysiaDocumento110 páginas7 Case Definitions of Infectious Disease in MalaysiaICAún no hay calificaciones
- TP-L3-402 Nursing Admin Checklist 5.1Documento2 páginasTP-L3-402 Nursing Admin Checklist 5.1عبيدة محمد ابو عابدAún no hay calificaciones
- Uniprot IDs of spike proteins from coronaviruses and other virusesDocumento8 páginasUniprot IDs of spike proteins from coronaviruses and other virusesPiyush RajAún no hay calificaciones
- Municipal Order Designates Anti-Drug Abuse Council Focal PersonsDocumento1 páginaMunicipal Order Designates Anti-Drug Abuse Council Focal Personscamille quezonAún no hay calificaciones
- Mechanical Paque RemovalDocumento16 páginasMechanical Paque RemovalMihaiAún no hay calificaciones
- WHO 2019 nCoV Vaccination Microplanning 2021.1 EngDocumento81 páginasWHO 2019 nCoV Vaccination Microplanning 2021.1 Engdr.tabitaAún no hay calificaciones
- Barriers To NP Practice That Impact Healthcare RedesignDocumento15 páginasBarriers To NP Practice That Impact Healthcare RedesignMartini ListrikAún no hay calificaciones
- Dr. Purnanti KipnandariDocumento54 páginasDr. Purnanti KipnandariFathzcepholapotz Tjah InsyafAún no hay calificaciones
- NUR091 - Session 8Documento6 páginasNUR091 - Session 8aquinoemjay27Aún no hay calificaciones
- Duties and Responsibilities of Chief Medical OfficerDocumento18 páginasDuties and Responsibilities of Chief Medical OfficerkgnmatinAún no hay calificaciones
- Pathology Item CardDocumento2 páginasPathology Item CardBir Mohammad SonetAún no hay calificaciones
- DOH STANDARDS (Indicators) For LEVEL 2 HOSPITALDocumento55 páginasDOH STANDARDS (Indicators) For LEVEL 2 HOSPITALMOHBARMM PlanningStaffAún no hay calificaciones
- Illinois Contract Amendment 092016Documento230 páginasIllinois Contract Amendment 092016Olly NubarAún no hay calificaciones
- Cervical Insufficiency:: Miscarriage Early (Premature)Documento2 páginasCervical Insufficiency:: Miscarriage Early (Premature)Ardelean EmanuelAún no hay calificaciones
- Daftar Pustaka: Poltekkes Kemenkes YogyakartaDocumento6 páginasDaftar Pustaka: Poltekkes Kemenkes YogyakartaNurhadi KebluksAún no hay calificaciones
- WHO WPE GIH 2020.2 Eng PDFDocumento11 páginasWHO WPE GIH 2020.2 Eng PDFMaicon MarquesAún no hay calificaciones
- Healthcare Disinfection and Sterilization GuideDocumento8 páginasHealthcare Disinfection and Sterilization GuideAyu AndrianiAún no hay calificaciones
- First Aid NewDocumento47 páginasFirst Aid Newchristopher100% (1)
- Quality, Costs, and Policy Factors InfluencingDocumento1 páginaQuality, Costs, and Policy Factors InfluencingRubi ZimmermanAún no hay calificaciones
- Nursing Home Checklist: Basic Information Yes No NotesDocumento9 páginasNursing Home Checklist: Basic Information Yes No NotesHarendra Narayan Singh100% (1)
- Case Study Bronchial Asthma-1Documento13 páginasCase Study Bronchial Asthma-1Krishna Krishii AolAún no hay calificaciones
- Wash in School ProgramDocumento12 páginasWash in School ProgramSDO MedicalAún no hay calificaciones
- Glycemic Targets 2022Documento14 páginasGlycemic Targets 2022Tom BiusoAún no hay calificaciones
- Path Fit100: Physical Activities Towrds Health and Fitness Movement CompetencyDocumento1 páginaPath Fit100: Physical Activities Towrds Health and Fitness Movement CompetencyChristian Fel MoralitaAún no hay calificaciones
- Clinical Practice Guidelines for Hepatitis B Virus (HBV) ManagementDocumento48 páginasClinical Practice Guidelines for Hepatitis B Virus (HBV) ManagementAqila MumtazAún no hay calificaciones