También podría gustarte
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Jurnal PneumoniaDocumento2 páginasJurnal PneumoniaSafira R. AissyAún no hay calificaciones
- ChleraDocumento26 páginasChleraadelekeyusufAún no hay calificaciones
- Sexually Transmitted DiseasesDocumento9 páginasSexually Transmitted DiseasesRodrigo Paolo Marquina EscuadraAún no hay calificaciones
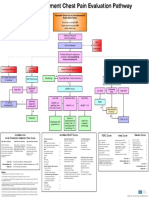
- Emergency Department Chest Pain Evaluation PathwayDocumento2 páginasEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidAún no hay calificaciones
- 11 - Precautions For Handling Organic SolventDocumento2 páginas11 - Precautions For Handling Organic SolventMummy TheAún no hay calificaciones
- Board 4-CHNDocumento30 páginasBoard 4-CHNKira100% (22)
- Conjunctivitis A Systematic Review of Diagnosis and TreatmentDocumento18 páginasConjunctivitis A Systematic Review of Diagnosis and TreatmentdasityarachmanAún no hay calificaciones
- NP 1 - Board of NursingDocumento34 páginasNP 1 - Board of NursingGo IdeasAún no hay calificaciones
- Raktapitta With Reference To Thrombocytopenia A Conceptual StudyDocumento4 páginasRaktapitta With Reference To Thrombocytopenia A Conceptual StudyEditor IJTSRDAún no hay calificaciones
- Revista Gastroenterologia Mexico: Scientific LetterDocumento4 páginasRevista Gastroenterologia Mexico: Scientific LetterPriyanshu SinghAún no hay calificaciones
- Gastroenterology and Hepatology Test RequestDocumento4 páginasGastroenterology and Hepatology Test Requestbassam alharaziAún no hay calificaciones
- Trigger FingerDocumento1 páginaTrigger FingerWisniardhy Suarnata PradanaAún no hay calificaciones
- Anaesthesia & Intensive Care: For Fcai, Frca EdaicDocumento139 páginasAnaesthesia & Intensive Care: For Fcai, Frca EdaicMuhammad Farid100% (2)
- NCPDocumento7 páginasNCPJulianne Jeamer FabroaAún no hay calificaciones
- SECOND YEAR PHARMD Syllabus PU PDFDocumento14 páginasSECOND YEAR PHARMD Syllabus PU PDFRIYA ROYAún no hay calificaciones
- Acu PressureDocumento26 páginasAcu PressureMuthuvel M100% (4)
- Case Study PresentationDocumento21 páginasCase Study Presentationapi-272776993Aún no hay calificaciones
- ANALGESICsDocumento30 páginasANALGESICsWan Hazmirul100% (1)
- Understanding & Practices of Weight ManagementDocumento445 páginasUnderstanding & Practices of Weight ManagementOnlineGatha The Endless TaleAún no hay calificaciones
- Biers BlockDocumento4 páginasBiers Blockemkay1234Aún no hay calificaciones
- Neuroimaging Self Assessment Colour ReviewDocumento228 páginasNeuroimaging Self Assessment Colour ReviewHamza Arjah100% (1)
- Analytical Exposition TextDocumento2 páginasAnalytical Exposition TextastridAún no hay calificaciones
- Bethel Schools 2018-2019 CalendarDocumento1 páginaBethel Schools 2018-2019 CalendarSinclair Broadcast Group - EugeneAún no hay calificaciones
- Healing Siddha Medicine-LibreDocumento4 páginasHealing Siddha Medicine-LibreVijay ShanmugasundaramAún no hay calificaciones
- 6 SepDocumento24 páginas6 SepKlinik PejatenAún no hay calificaciones
- Respiratory SystemDocumento16 páginasRespiratory Systemapi-277775953Aún no hay calificaciones
- Mood Disorders StudentDocumento32 páginasMood Disorders StudentRafly FernandaAún no hay calificaciones
- 1 - RF Report ?Documento3 páginas1 - RF Report ?مدى القحطانيAún no hay calificaciones
- SucralfateDocumento3 páginasSucralfateViziteu AlexandraAún no hay calificaciones
- Spritual Health Life: 1. Gyan Mudra (Mudra of Knowledge)Documento10 páginasSpritual Health Life: 1. Gyan Mudra (Mudra of Knowledge)chachu123100% (2)