También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (895)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2104)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Immunology Exam Q's With AnswersDocumento26 páginasImmunology Exam Q's With AnswersHavardKrovel87% (55)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- @MedicalBooksStore 2014 Best of PDFDocumento284 páginas@MedicalBooksStore 2014 Best of PDFSaman SarKoAún no hay calificaciones
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- ScienceGeography3ResourceSample PDFDocumento9 páginasScienceGeography3ResourceSample PDFmargantoniAún no hay calificaciones
- Blistering DisordersDocumento7 páginasBlistering DisordersSaman SarKoAún no hay calificaciones
- 1536106348Documento144 páginas1536106348Saman SarKoAún no hay calificaciones
- Canuuc Ed Revisions May 2017Documento37 páginasCanuuc Ed Revisions May 2017Saman SarKoAún no hay calificaciones
- @MBS MedicalBooksStore 2019 Management PDFDocumento310 páginas@MBS MedicalBooksStore 2019 Management PDFSaman SarKo100% (2)
- The Blood Supply of EsophagusDocumento4 páginasThe Blood Supply of EsophagusSaman SarKoAún no hay calificaciones
- Geriatric Medicine: Biology of AgeingDocumento6 páginasGeriatric Medicine: Biology of AgeingSaman SarKoAún no hay calificaciones
- Abnormal LabourDocumento7 páginasAbnormal LabourSaman SarKo0% (1)
- AnthraxDocumento5 páginasAnthraxSaman SarKoAún no hay calificaciones
- Amniotic Fluid and ItDocumento8 páginasAmniotic Fluid and ItSaman SarKoAún no hay calificaciones
- Acute AppendixDocumento16 páginasAcute AppendixSaman SarKoAún no hay calificaciones
- Dr. Lujain Alkhazrajy: Acquired Immune Deficiency Syndrome (AIDS)Documento11 páginasDr. Lujain Alkhazrajy: Acquired Immune Deficiency Syndrome (AIDS)Saman SarKoAún no hay calificaciones
- Peripheral Nerve DisorderDocumento23 páginasPeripheral Nerve DisorderSaman SarKoAún no hay calificaciones
- Acquired Heart DiseasesDocumento41 páginasAcquired Heart DiseasesSaman SarKoAún no hay calificaciones
- Skeletal System: I. General CharacteristicsDocumento34 páginasSkeletal System: I. General CharacteristicsMason BruceAún no hay calificaciones
- An Updated Approach To The Diagnosis of Myeloid Leukemia CutisDocumento10 páginasAn Updated Approach To The Diagnosis of Myeloid Leukemia CutisfikriafisAún no hay calificaciones
- IB Singh Vol-2Documento387 páginasIB Singh Vol-2dannyAún no hay calificaciones
- Ai Chi - Meridians2Documento4 páginasAi Chi - Meridians2sale18100% (1)
- Reproductive SystemDocumento49 páginasReproductive SystemAyro Business CenterAún no hay calificaciones
- 2020 Pathology Compilation Questions by TopicsDocumento7 páginas2020 Pathology Compilation Questions by Topicsrupertgrint2000Aún no hay calificaciones
- Anatomy Chapters 6&7Documento17 páginasAnatomy Chapters 6&7Tamara IdalyAún no hay calificaciones
- Appearances - How To Describe Someone in EnglishDocumento26 páginasAppearances - How To Describe Someone in EnglishNadia Tara DilaAún no hay calificaciones
- Physiology of Hemostasis - Dr. Rahmat Dani Satria PH.D., SP - PK (K)Documento27 páginasPhysiology of Hemostasis - Dr. Rahmat Dani Satria PH.D., SP - PK (K)Viand NugrohoAún no hay calificaciones
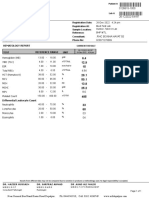
- BILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationDocumento1 páginaBILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationsaifAún no hay calificaciones
- Chapter 13 Surgical Managment of Salivary Gland DiseaseDocumento35 páginasChapter 13 Surgical Managment of Salivary Gland DiseaseMohammed Qasim Al-WataryAún no hay calificaciones
- Cytophysiology Revised 2014Documento19 páginasCytophysiology Revised 2014Julienne Sanchez-SalazarAún no hay calificaciones
- Mitosis PresentationDocumento24 páginasMitosis Presentationapi-267309851Aún no hay calificaciones
- Floyd17 TB Ch12Documento5 páginasFloyd17 TB Ch12sdjuknicAún no hay calificaciones
- Chapter 12: The Back: Vertebral ColumnDocumento7 páginasChapter 12: The Back: Vertebral ColumnJyrra NeriAún no hay calificaciones
- Human Body Temperature and New Approaches To ConstDocumento21 páginasHuman Body Temperature and New Approaches To ConstCarlos Apodman BellaAún no hay calificaciones
- Physiology of Reproduction in Women IDocumento34 páginasPhysiology of Reproduction in Women Iapi-196413370% (1)
- Disorders of Red Blood CellsDocumento27 páginasDisorders of Red Blood Cellskirti sharmaAún no hay calificaciones
- Histologie Généralité Et Tissu Epithelume PDFDocumento2 páginasHistologie Généralité Et Tissu Epithelume PDFشكوب ستانAún no hay calificaciones
- Anatomy AND Physiology: The Human As An OrganismsDocumento26 páginasAnatomy AND Physiology: The Human As An OrganismsJake Donely C. PaduaAún no hay calificaciones
- Cavidades Corporales AnatomiaDocumento4 páginasCavidades Corporales AnatomiaBOKOR5000Aún no hay calificaciones
- Cervical and Shoulder 2020Documento14 páginasCervical and Shoulder 2020Eduardo OlivaAún no hay calificaciones
- Human Anatomy Lab Manual 1612818025. - PrintDocumento219 páginasHuman Anatomy Lab Manual 1612818025. - Printmishraadityaraj516Aún no hay calificaciones
- CytoskeletonDocumento86 páginasCytoskeletonAbid Al RezaAún no hay calificaciones
- Hemorrhagic Conditions of Late Pregnancy Other Related Problems 1Documento5 páginasHemorrhagic Conditions of Late Pregnancy Other Related Problems 1imnasAún no hay calificaciones
- Digestive SystemDocumento45 páginasDigestive SystemEzequiel ManluluAún no hay calificaciones
- Bio Mechanics of Spinal ColumnDocumento59 páginasBio Mechanics of Spinal ColumnOnwaree Ing100% (4)
- WORKSHEET 11.1 Locomotion and Support in Humans and AnimalsDocumento7 páginasWORKSHEET 11.1 Locomotion and Support in Humans and AnimalsSakinah RahimAún no hay calificaciones