También podría gustarte
- Accurate Optical Biometry Using IOL MasterDocumento5 páginasAccurate Optical Biometry Using IOL Mastermuzicka9Aún no hay calificaciones
- The Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersDe EverandThe Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersAún no hay calificaciones
- Tinted Lens in Low VisionDocumento10 páginasTinted Lens in Low VisionAmrit PokharelAún no hay calificaciones
- Angulo KappaDocumento8 páginasAngulo KappaLívia Duarte Pimentel Vinhadelli100% (1)
- Corneal Cross-Linking: Treatment for Cornea DiseaseDe EverandCorneal Cross-Linking: Treatment for Cornea DiseaseAún no hay calificaciones
- Pentacam Guideline 3rd 0218 KDocumento220 páginasPentacam Guideline 3rd 0218 KHarshit RajputAún no hay calificaciones
- 1.ocular Biometry (Full) SEGi UDocumento51 páginas1.ocular Biometry (Full) SEGi UDiana PhiriAún no hay calificaciones
- The Skeffington Perspective of the Behavioral Model of Optometric Data Analysis and Vision CareDe EverandThe Skeffington Perspective of the Behavioral Model of Optometric Data Analysis and Vision CareAún no hay calificaciones
- Zernike Polynomials and Their Use in Describing The Wavefront Aberrations of The Human EyeDocumento24 páginasZernike Polynomials and Their Use in Describing The Wavefront Aberrations of The Human EyeRadixMonsAún no hay calificaciones
- Posterior Polar Cataract Management: My Approach: 2022, #1De EverandPosterior Polar Cataract Management: My Approach: 2022, #1Aún no hay calificaciones
- Clinical Study On Scleral Lenses by Dr. Elise KramerDocumento8 páginasClinical Study On Scleral Lenses by Dr. Elise KramerMiami Contact Lens InstituteAún no hay calificaciones
- IOL PowerDocumento273 páginasIOL Powermarlon García100% (2)
- Recent Advances in Laser Refractive SurgeryDocumento24 páginasRecent Advances in Laser Refractive SurgeryKPJConferenceAún no hay calificaciones
- Scientific Foundations of OphthalmologyDe EverandScientific Foundations of OphthalmologyEdward S. PerkinsAún no hay calificaciones
- Continue: Stallard's Eye Surgery PDFDocumento3 páginasContinue: Stallard's Eye Surgery PDFCod Mobile100% (1)
- Contact Applanation TonometryDocumento6 páginasContact Applanation TonometryAmirhosseinSamadzadehAún no hay calificaciones
- Belin Ambrosio Enhanced Ectasia DetectionDocumento8 páginasBelin Ambrosio Enhanced Ectasia DetectionClaudio Castillo SandovalAún no hay calificaciones
- CH0MO0038s2007 PDFDocumento103 páginasCH0MO0038s2007 PDFJulie Damiles-Aguilar BibbiganAún no hay calificaciones
- Glaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913De EverandGlaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913Aún no hay calificaciones
- CPG 19Documento78 páginasCPG 19anon-24970100% (1)
- A Critical Evaluation of The Evidence Supporting The Practice Behavioral Vision TherapyDocumento23 páginasA Critical Evaluation of The Evidence Supporting The Practice Behavioral Vision TherapyPierre A. RodulfoAún no hay calificaciones
- Ectasia Screening With PentacamDocumento9 páginasEctasia Screening With Pentacamkurosaki_1974Aún no hay calificaciones
- MASTER'S GUIDE TO Manual SICSDocumento192 páginasMASTER'S GUIDE TO Manual SICSAndri SaputraAún no hay calificaciones
- Care & Maintenance of Contact LenseDocumento26 páginasCare & Maintenance of Contact LenseGurria NaheedAún no hay calificaciones
- The Evolution of The Ophthalmic Surgical MicroscopeDocumento33 páginasThe Evolution of The Ophthalmic Surgical MicroscopeSai Naga Sri HarshaAún no hay calificaciones
- Fundamentals of RetinosDocumento51 páginasFundamentals of RetinosJelshan BawogbogAún no hay calificaciones
- Foreign Optometrist For CanadaDocumento9 páginasForeign Optometrist For CanadaABDUL HAMEEDAún no hay calificaciones
- Wills Eye ManualDocumento2 páginasWills Eye ManualKeyko Lampita33% (3)
- Case Studies PresbyopiaDocumento33 páginasCase Studies PresbyopiaMalaika ZubairAún no hay calificaciones
- Glaucoma Medical Therapy PDFDocumento313 páginasGlaucoma Medical Therapy PDFJihan RuhiAún no hay calificaciones
- Ophthalmology: Current and Future Developments: Volume 2: Diagnostic Atlas of Retinal DiseasesDe EverandOphthalmology: Current and Future Developments: Volume 2: Diagnostic Atlas of Retinal DiseasesAún no hay calificaciones
- PERIMETRY Introduction GuideDocumento70 páginasPERIMETRY Introduction GuideDana Andreea Popescu100% (1)
- NATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideDe EverandNATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideAún no hay calificaciones
- Job Description of A Trained and Registered Ophthalmic NurseDocumento1 páginaJob Description of A Trained and Registered Ophthalmic NurseKwaku OwusuAún no hay calificaciones
- Walds Visual CycleDocumento12 páginasWalds Visual CycleSambit DashAún no hay calificaciones
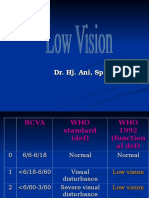
- Low VisionDocumento36 páginasLow VisionIqbal HabibieAún no hay calificaciones
- Optometry PresentationDocumento11 páginasOptometry PresentationEvelyn Tran100% (1)
- Angle Closure Glaucoma PDFDocumento289 páginasAngle Closure Glaucoma PDFsisil muntheAún no hay calificaciones
- The Optical Quality of The CorneaDocumento32 páginasThe Optical Quality of The CorneaacalossiAún no hay calificaciones
- HBN 12 Supl4 PDFDocumento76 páginasHBN 12 Supl4 PDFpanteaAún no hay calificaciones
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsDe EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsAún no hay calificaciones
- Issues in Ophthalmic Practice: Current and future challengesDe EverandIssues in Ophthalmic Practice: Current and future challengesCalificación: 4.5 de 5 estrellas4.5/5 (2)
- Refractive SurgeryDocumento86 páginasRefractive Surgeryrvnkrish24100% (3)
- 120217gsaarticlefinal3 PDFDocumento4 páginas120217gsaarticlefinal3 PDFItmam MilatakaAún no hay calificaciones
- 0210 IOL HandbookDocumento15 páginas0210 IOL HandbookHombre69Aún no hay calificaciones
- Femto Laser in OphthalmologyDocumento11 páginasFemto Laser in Ophthalmologylycan007Aún no hay calificaciones
- Night MiopiaDocumento8 páginasNight MiopiamurilobsouzaAún no hay calificaciones
- Basic Sciences in Ophthalmology - 9788184486087-EmailDocumento446 páginasBasic Sciences in Ophthalmology - 9788184486087-EmailwulanfarichahAún no hay calificaciones
- International Council of Ophthalmology's Ophthalmology Surgical Competency Assessment Rubrics (ICO-OSCAR)Documento4 páginasInternational Council of Ophthalmology's Ophthalmology Surgical Competency Assessment Rubrics (ICO-OSCAR)zaidoonys1Aún no hay calificaciones
- Clinical Optics: Basic and Clinical Science CourseDocumento18 páginasClinical Optics: Basic and Clinical Science CourseIlham SamodraAún no hay calificaciones
- Ophthalmic Ultrasound Jaypee Gold Standard Mini Atlas Series®Documento315 páginasOphthalmic Ultrasound Jaypee Gold Standard Mini Atlas Series®Elizabeth SantosAún no hay calificaciones
- Cycloplegic Retinoscopy in InfancyDocumento5 páginasCycloplegic Retinoscopy in InfancyStrauss de LangeAún no hay calificaciones
- InTech-Pressure Lowering MedicationsDocumento32 páginasInTech-Pressure Lowering MedicationsriveliAún no hay calificaciones
- Boyd - Practical Aspects of Laser Photocoagulation - CH 6Documento16 páginasBoyd - Practical Aspects of Laser Photocoagulation - CH 6riveliAún no hay calificaciones
- The Future of Diabetic Retinopathy TreatmentDocumento4 páginasThe Future of Diabetic Retinopathy TreatmentriveliAún no hay calificaciones
- Combination Therapy For Diffuse DMEDocumento2 páginasCombination Therapy For Diffuse DMEriveliAún no hay calificaciones
- Emedicine - Albinism - OculocutaneousDocumento10 páginasEmedicine - Albinism - OculocutaneousriveliAún no hay calificaciones
- CH42 Management of Complicated Retinal DetachmentDocumento36 páginasCH42 Management of Complicated Retinal DetachmentriveliAún no hay calificaciones
- Hypertensive Retinopathy - Yanoff and DukerDocumento13 páginasHypertensive Retinopathy - Yanoff and DukerriveliAún no hay calificaciones
- Emedicine - Acute Rheumatic Fever Article by Robert J MeadDocumento21 páginasEmedicine - Acute Rheumatic Fever Article by Robert J MeadriveliAún no hay calificaciones
- Complications of Diabetic Vitreoretinal Surgery - A ReviewDocumento4 páginasComplications of Diabetic Vitreoretinal Surgery - A ReviewriveliAún no hay calificaciones
- Anterior Chamber Angle Assessment Technique - CH 17Documento20 páginasAnterior Chamber Angle Assessment Technique - CH 17riveliAún no hay calificaciones
- The Physical Examination of The EyeDocumento16 páginasThe Physical Examination of The EyeriveliAún no hay calificaciones
- Emedicine - Actinomycosis. MBG.Documento8 páginasEmedicine - Actinomycosis. MBG.riveliAún no hay calificaciones
- Steps For A Safe Intravitreal Injection Technique - A ReviewDocumento6 páginasSteps For A Safe Intravitreal Injection Technique - A ReviewriveliAún no hay calificaciones
- Lens Management For VitrectomyDocumento4 páginasLens Management For VitrectomyriveliAún no hay calificaciones
- Lens Management For VitrectomyDocumento4 páginasLens Management For VitrectomyriveliAún no hay calificaciones
- Postoperative Complication of Periocular AnesthesiaDocumento7 páginasPostoperative Complication of Periocular AnesthesiariveliAún no hay calificaciones
- Measures of Central TendencyDocumento9 páginasMeasures of Central TendencyriveliAún no hay calificaciones
- InTech - ElectroretinogramsDocumento250 páginasInTech - ElectroretinogramsriveliAún no hay calificaciones
- InTech - Clinical Applications of Optical Coherence Tomography in OphthalmologyDocumento42 páginasInTech - Clinical Applications of Optical Coherence Tomography in OphthalmologyriveliAún no hay calificaciones
- Hypothesis PracticeDocumento9 páginasHypothesis PracticeriveliAún no hay calificaciones
- Surgical Pearls For The Beginning Vitreoretinal FellowDocumento3 páginasSurgical Pearls For The Beginning Vitreoretinal FellowriveliAún no hay calificaciones
- Postoperative Complication of Periocular AnesthesiaDocumento7 páginasPostoperative Complication of Periocular AnesthesiariveliAún no hay calificaciones
- Postoperative Sympatethic OphthalmologyDocumento11 páginasPostoperative Sympatethic OphthalmologyriveliAún no hay calificaciones
- Populations, Distributions and SamplesDocumento4 páginasPopulations, Distributions and SamplesriveliAún no hay calificaciones
- 465Documento3 páginas465riveliAún no hay calificaciones
- Glaucoma NotesDocumento39 páginasGlaucoma NotesMuhammad SabirAún no hay calificaciones
- George Asimellis - Visual Optics (Lectures in Optics, 4) 4 (2022, SPIE Press)Documento722 páginasGeorge Asimellis - Visual Optics (Lectures in Optics, 4) 4 (2022, SPIE Press)EUGEN100% (1)
- Diurnal Variations in Intraocular PressureDocumento34 páginasDiurnal Variations in Intraocular PressureAgung DarmawanAún no hay calificaciones
- Soft Contact Lens Complicatioan - EditedDocumento41 páginasSoft Contact Lens Complicatioan - EditedR.m. AndriyanAún no hay calificaciones
- Diagnostic and History Taking 诊断和病史Documento48 páginasDiagnostic and History Taking 诊断和病史Devi NurpitaAún no hay calificaciones
- SquintDocumento7 páginasSquintasmaelgathafiAún no hay calificaciones
- Dynamic RetinosDocumento6 páginasDynamic RetinosguybarnettAún no hay calificaciones
- Clinical Examination - OphthalmologyDocumento18 páginasClinical Examination - OphthalmologyMohammed EsmailAún no hay calificaciones
- Oculus: Pentacam Pentacam HRDocumento20 páginasOculus: Pentacam Pentacam HRSaecio OpticoAún no hay calificaciones
- RIZALDocumento3 páginasRIZALJed Daet0% (1)
- The Wordsley Step Incision For Axillary Lymph-Node DissectionDocumento1 páginaThe Wordsley Step Incision For Axillary Lymph-Node DissectionVlad GrigoreAún no hay calificaciones
- ENT - Ear-Nose-Throat PDFDocumento15 páginasENT - Ear-Nose-Throat PDFMa SakhiAún no hay calificaciones
- Sjogren SyndromeDocumento58 páginasSjogren SyndromeKarina BudijantoAún no hay calificaciones
- Subjective Refraction Mark RosenfieldDocumento19 páginasSubjective Refraction Mark RosenfieldWendy RodriguezAún no hay calificaciones
- COF Rubin GeldenhuysDocumento1 páginaCOF Rubin GeldenhuysRubin GeldenhuysAún no hay calificaciones
- McKees Pathology of The SkinDocumento1819 páginasMcKees Pathology of The Skincatalink2191% (11)
- Ebook Advances in Ophthalmology and Optometry 2022 Volume 7 1 Advances Volume 7 1 PDF Full Chapter PDFDocumento67 páginasEbook Advances in Ophthalmology and Optometry 2022 Volume 7 1 Advances Volume 7 1 PDF Full Chapter PDFleigh.harrison612100% (17)
- Epidemiology of Keratoconus Symposium: KeratoconusDocumento2 páginasEpidemiology of Keratoconus Symposium: KeratoconusdechastraAún no hay calificaciones
- Keratoconus Screening Using Values Derived From Auto-Keratometer Measurements: A Multicenter StudyDocumento8 páginasKeratoconus Screening Using Values Derived From Auto-Keratometer Measurements: A Multicenter Study小島隆司Aún no hay calificaciones
- Muscles of The EyeDocumento3 páginasMuscles of The EyeAnna GarbiAún no hay calificaciones
- Refraction Handbook For CliniciansDocumento20 páginasRefraction Handbook For CliniciansDoina Bobescu0% (1)
- Management of Corneal Ulcer PDFDocumento2 páginasManagement of Corneal Ulcer PDFYosiita KartinaaAún no hay calificaciones
- Phy Viii Ch.16 Light Assignment Ankur SharmaDocumento5 páginasPhy Viii Ch.16 Light Assignment Ankur SharmaAtharv ChauhanAún no hay calificaciones
- Intraocular Inflammation 2016 PDFDocumento1530 páginasIntraocular Inflammation 2016 PDFAura-Nicoleta PopinciucAún no hay calificaciones
- ICSE Class X Sense Organs NotesDocumento26 páginasICSE Class X Sense Organs Notesprogrammer.ron.akAún no hay calificaciones
- IAPB 08 PosterDocumento1 páginaIAPB 08 Postertovih27684Aún no hay calificaciones
- What Is AstigmatismDocumento6 páginasWhat Is AstigmatismMernie Grace DionesioAún no hay calificaciones
- Macular Function TestDocumento2 páginasMacular Function TestNeha SinghAún no hay calificaciones
- OrthopticDocumento9 páginasOrthopticSobiafarooqAún no hay calificaciones
- Tampil Cantik Dengan Eyes RejuvenationDocumento33 páginasTampil Cantik Dengan Eyes RejuvenationBidang Keperawatan RswbAún no hay calificaciones