También podría gustarte
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeCalificación: 4 de 5 estrellas4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceCalificación: 4 de 5 estrellas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Calificación: 4 de 5 estrellas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureCalificación: 4.5 de 5 estrellas4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDe EverandShoe Dog: A Memoir by the Creator of NikeCalificación: 4.5 de 5 estrellas4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaCalificación: 4.5 de 5 estrellas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe EverandThe Little Book of Hygge: Danish Secrets to Happy LivingCalificación: 3.5 de 5 estrellas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe EverandNever Split the Difference: Negotiating As If Your Life Depended On ItCalificación: 4.5 de 5 estrellas4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe EverandGrit: The Power of Passion and PerseveranceCalificación: 4 de 5 estrellas4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryCalificación: 3.5 de 5 estrellas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe EverandThe Emperor of All Maladies: A Biography of CancerCalificación: 4.5 de 5 estrellas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe EverandTeam of Rivals: The Political Genius of Abraham LincolnCalificación: 4.5 de 5 estrellas4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe EverandOn Fire: The (Burning) Case for a Green New DealCalificación: 4 de 5 estrellas4/5 (72)
- The Unwinding: An Inner History of the New AmericaDe EverandThe Unwinding: An Inner History of the New AmericaCalificación: 4 de 5 estrellas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersCalificación: 4.5 de 5 estrellas4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDe EverandRise of ISIS: A Threat We Can't IgnoreCalificación: 3.5 de 5 estrellas3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyCalificación: 3.5 de 5 estrellas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreCalificación: 4 de 5 estrellas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Calificación: 4.5 de 5 estrellas4.5/5 (119)
- The Perks of Being a WallflowerDe EverandThe Perks of Being a WallflowerCalificación: 4.5 de 5 estrellas4.5/5 (2099)
- Her Body and Other Parties: StoriesDe EverandHer Body and Other Parties: StoriesCalificación: 4 de 5 estrellas4/5 (821)
- Shear StrengthDocumento147 páginasShear StrengthZemen JMAún no hay calificaciones
- Chapter 2 Member DesignDocumento73 páginasChapter 2 Member Designbsitler100% (2)
- Quality Management System for Installation of UPVC PipesDocumento1 páginaQuality Management System for Installation of UPVC PipesRajput AmitAún no hay calificaciones
- Solar Water Purifier 2D DrawingsDocumento4 páginasSolar Water Purifier 2D DrawingsMurali DathanAún no hay calificaciones
- C# .NET CoreDocumento707 páginasC# .NET CoreKevin Moreira100% (1)
- ISO 5554-1978 - Determinação Do Teor de AmidoDocumento12 páginasISO 5554-1978 - Determinação Do Teor de AmidoJocilene DantasAún no hay calificaciones
- Liquid Nitrogen Filled Power TransformerDocumento6 páginasLiquid Nitrogen Filled Power TransformerHamayoun MurtazaAún no hay calificaciones
- 1!!! Microalgae and Wastewater Treatment PDFDocumento19 páginas1!!! Microalgae and Wastewater Treatment PDFAhmadAún no hay calificaciones
- T4-04 Qs PAPER SAMDocumento3 páginasT4-04 Qs PAPER SAMAman SaxenaAún no hay calificaciones
- Operator'S Manual Px15P-Xxx-Xxx-Axxx: 1-1/2" Diaphragm PumpDocumento12 páginasOperator'S Manual Px15P-Xxx-Xxx-Axxx: 1-1/2" Diaphragm PumpNashrullah AhmadAún no hay calificaciones
- Simulink TutorialDocumento15 páginasSimulink Tutorialsukhbir24Aún no hay calificaciones
- Metric Socket Head Cap Screws1 PDFDocumento2 páginasMetric Socket Head Cap Screws1 PDFRavi BabaladiAún no hay calificaciones
- KCP Solar Brochure PDFDocumento2 páginasKCP Solar Brochure PDFSharad MishraAún no hay calificaciones
- Terms of Reference (Consultancy PSHS Zamboanga Peninsula)Documento8 páginasTerms of Reference (Consultancy PSHS Zamboanga Peninsula)Arniel LaguardiaAún no hay calificaciones
- USE THE BEST fire suppression coatingDocumento4 páginasUSE THE BEST fire suppression coatingTamba PasaribuAún no hay calificaciones
- Interior Fluid Resistant Epoxy Primer: Technical Data SheetDocumento5 páginasInterior Fluid Resistant Epoxy Primer: Technical Data SheetLeonard Ngiam YkAún no hay calificaciones
- Acco Chain CatalogDocumento75 páginasAcco Chain CatalogVIVEK YADAVAún no hay calificaciones
- Supplier Document Cover Page: Greater Enfield Subsea EPCIDocumento16 páginasSupplier Document Cover Page: Greater Enfield Subsea EPCIKarthikeyan GanesanAún no hay calificaciones
- Lighting Catalog AppletonDocumento796 páginasLighting Catalog AppletonAlejandro Araneda Albornoz100% (1)
- Rail CorrosionDocumento71 páginasRail CorrosionkishanrwtAún no hay calificaciones
- Introduction To Fires and ExplosionsDocumento21 páginasIntroduction To Fires and Explosionssalman1111aAún no hay calificaciones
- Surveying Work Method StatementDocumento5 páginasSurveying Work Method StatementKelvin TanAún no hay calificaciones
- Parts ListDocumento15 páginasParts ListAstraluxAún no hay calificaciones
- Certificate of Calibration: Customer InformationDocumento2 páginasCertificate of Calibration: Customer InformationSazzath HossainAún no hay calificaciones
- Fluent UdfDocumento2 páginasFluent UdfArvind MuraliAún no hay calificaciones
- NITdw 21Documento15 páginasNITdw 21Kartik JoshiAún no hay calificaciones
- Https-::images Homedepot-Static Com:catalog:pdfimages:01Documento5 páginasHttps-::images Homedepot-Static Com:catalog:pdfimages:01droopyboreAún no hay calificaciones
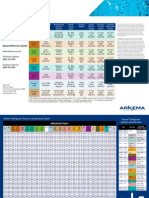
- Retrofitting With Forane Quickrefguide FinalDocumento2 páginasRetrofitting With Forane Quickrefguide FinalCoolSolutions ElSalvadorAún no hay calificaciones
- 1802 04173 PDFDocumento87 páginas1802 04173 PDFÇhura CristianAún no hay calificaciones
- C-Steel Composited (E70C-3M, E70C-6M) PDFDocumento2 páginasC-Steel Composited (E70C-3M, E70C-6M) PDFborovniskiAún no hay calificaciones